Psychology is rooted in science that seeks to understand our thoughts, feelings and actions. It is also a broad field – some psychology professionals develop and test theories through basic research; while others work to help individuals, organizations, and communities better function; still others are both researchers and practitioners.
Profiles
 The theme of Psychology Month 2026 was “This Is Psychology”. It highlighted the ways psychology has something to contribute and something to say about most every issue that affects Canadians, big and small. That wide swath of knowledge and expertise is remarkable, and in today’s uncertain world it is invaluable. Psychology, and psychologists, have an opportunity to be instrumental in moving the world, and our country, toward positive, lasting, and evidence-based change. Now is the time to do it.
The theme of Psychology Month 2026 was “This Is Psychology”. It highlighted the ways psychology has something to contribute and something to say about most every issue that affects Canadians, big and small. That wide swath of knowledge and expertise is remarkable, and in today’s uncertain world it is invaluable. Psychology, and psychologists, have an opportunity to be instrumental in moving the world, and our country, toward positive, lasting, and evidence-based change. Now is the time to do it.
Visit our 2026 Psychology Month page.
This month, in their Monitor on Psychology magazine, the American Psychological Association published an article called ‘Storytelling strengthens the impact of psychological science’ by Tori DeAngelis. It opens with the words “psychology is perhaps the science discipline best positioned to help people navigate 2026’s complexities”. It makes a point about how vital it is that psychologists share their findings, and why they matter, in a way that connects with large numbers of people.
I had this article in the back of my mind throughout Psychology Month this year, because it has a similar thesis to our theme of “This Is Psychology”. That being that psychological science, more than most any other scientific discipline, has something to contribute in nearly every facet of our everyday lives. And communicating that to the public, to decision-makers in organizations, and to policy-makers in government, is imperative.
Just knowing something shouldn’t be an end unto itself. There is little point in accruing knowledge if that knowledge doesn’t encourage positive change. Psychologists know, for example, that the Meyers-Briggs personality test is about as reliable and scientifically sound as astrology. And yet, it is used by all kinds of major companies in their hiring processes and in their internal organizational structures. In fact, it’s used by the majority of Fortune 500 companies, even though we (psychologists and those who research personality) know that the Big Five test is far more accurate.
Why do they keep doing it? Have we just not told them? Are they just ignoring the data that demonstrates the ineffectiveness of their method?
Here’s the thing – psychological science can inform a Fortune 500 company as to why using the Meyers-Briggs is a futile exercise. It can explain why that company is resistant to altering their practices. It can also show why that company might see benefits from what they’re currently doing even if the data doesn’t support those conclusions. It can even suggest ways that a person who wants to change that company’s practices can effectively make the case and be convincing about it.
The central problem, as I see it, is that of those various ways that psychology can contribute to that company’s work culture, efficiency, and even their bottom line, the weakest of them all is the most essential. We (although I am not a psychologist myself, I am going to use the word ‘we’ from here on out for the sake of convenience) are great at figuring out why people do things. We’re not so great at convincing them to do other things.
We nibble around the edges. We figure out ways to nudge people toward recycling more at their office, but we don’t have a great way to convince politicians to take significant action to fight climate change. We can tell the world that referring to youth by their chosen pronouns, and providing gender-affirming care to all people, has great health and wellness outcomes. We don’t have a great ability to convince school boards, governments, and the public to follow that science.
The thing is, we actually know how to do it! We study public response to rhetoric. We understand the way a message can be framed to have the greatest impact. Some of it is right there in the title of Ms. DeAngelis’ article. Storytelling strengthens the impact of psychological science. How do we have so much data on how to do it, but few of us want to be the ones who do?
Every year (and by that I mean last year and coming up again this year) I do a presentation at the CPA Convention with our incoming President, Dr. Janine Hubbard. It’s about speaking with the media, and I look at it as a call to members in the profession to get out there. My central message is usually to academics, and it is this – if not you, then who? People are going to be speaking about your area of expertise, but you are the expert.
Janine’s message is more one to practitioners (the psychologists who work in clinical practice and see patients). She points out that all psychologists do a lot of schooling, and know a heck of a lot about a lot of things. You may not be THE expert on post-traumatic stress, but you know enough to talk to the nice folks on the evening news about it for two minutes. You are equipped to provide the community with a little more understanding, and maybe a sense of comfort, in the aftermath of a tragedy. Most psychologists have some experience teaching students, and Janine thinks of a media appearance as an opportunity to teach the public about a subject. She draws on her experience as a child psychologist, explaining complex issues to kids and their parents on a regular basis. She says,
“All clinicians have to use appropriate language to meet their target audience. The same is true when reaching a larger audience.”
Janine herself kind of fell backward into this kind of work, and now not only has she become something of an expert at media appearances, she also sees the tremendous value they bring. A regular segment on the evening news in Newfoundland made her a familiar face in the community. That familiarity led to trust. That trust meant that Janine would be believed when she was speaking about something that really mattered.
People watch, and they listen. They listened to Janine when she talked about gender-affirming care. They listened when she talked about holiday stress, or the effects of the wildfires that terrified Newfoundland. And when she encouraged them to get vaccinated by talking them through needle fear, and encouraged them to follow public health guidelines by providing reassurances and sharing strategies to increase comfort with nasal swabs, viewers of the local news were indeed reassured. They trusted her credibility as a scientist, and as a familiar face.
I understand that this does not come naturally to many psychologists. It did not come naturally to Janine either, but recognizing the impact of doing it allowed her to grow into the role. I believe there are two effects from the scientific rigour that becomes second-nature to psychologists as they pursue their degrees.
One is a feeling that language must be extremely precise. They don’t feel comfortable saying, for example, that peeing when you’re not supposed to is far more common among five-year-olds than it is among 15-year-olds. Instead, they might have a tendency to say that enuresis affects between 5-10% of five-year-olds, and there is a difference between enuresis and nocturnal enuresis, and it happens in around 1% of 15-year-olds, but in their case it’s much more likely to be nocturnal…we know this kind of language loses listeners. But we would sometimes rather be precise than be heard. Thankfully, when she spoke to me for Psychology Month on the subject, Dr. Jen Theule drew on her experience explaining enuresis and encopresis (peeing and pooping where you shouldn’t) to children and explained it to me in a simple and straightforward way.
The second effect is the idea that when there is someone who knows something better than you know that thing, then it is not your place to speak about it. And if you do, the impostor syndrome metre starts peaking.
Janine told me a story once about trying to find other psychologists to do a segment on the news. She reached out to a number of her colleagues looking for someone to speak with a host, and all of them said no. It wasn’t their specific area of expertise, and they felt as though it was outside their scope, and so they declined. The subject they were being asked to speak about was impostor syndrome.
I say this to every psychologist I can. You know more about human behaviour, in most every aspect, than the people you will be able to reach by speaking up. I write about this discipline and psychological science, and have every day for the past six years. You still know more about every aspect of human behaviour than I do.
Almost two years ago, Dr. Steve Joordens wrote me to propose a podcast episode about the scourge of sports gambling. It was the first time I’d considered how dangerous online sports gambling really was for young people, and I was happy an immediately intrigued once Steve brought it to my attention. A short time later, Steve wrote a letter on behalf of the CPA, and soon would be speaking in front of the Senate to urge action on the advertising of sports gambling. He did a webinar for the CPA on the subject. He will be the guest editor for an upcoming behavioural-addiction-themed issue of the CPA magazine Psynopsis.
Steve is passionate about the dangers of gambling for youth. And in some ways he’s AN expert. He isn’t THE expert. But he knows more about it than most of the senators he was speaking to. And more than I know about it. THE expert might be Dr. Robert Sapolsky, and I know this because Steve had a little fanboy moment when meeting Dr. Sapolsky for the first time for this article we were working on for Psychology Month.
I, on the other hand, had never heard of Dr. Sapolsky before that moment. I suspect few psychologists would say the same. They might be as surprised to hear of my ignorance as I was when I found out my 26-year-old daughter had never heard of Bad Bunny before the Super Bowl. Dr. Sapolsky is, deservedly, a really big deal in psychology circles. But those circles are also bubbles. We all live in our own personal bubbles, and the psychology bubble is real.
In Ms. DeAngelis’ article, she quoted Dr. Myra Fernandes, a professor in cognitive neuroscience at the University of Waterloo in Canada and associate editor of the Canadian Journal of Experimental Psychology (CJEP), talking about how the journal system could do better connecting with the public. Dr. Fernandes says journals could require brief, lay-friendly public significance statements that explain a study in simple terms, including how it can benefit society. CJEP is one of the journals that asks for these statements, which is a good start. But an additional step is needed, I believe. That is one of intention.
When you publish that journal article, it’s entirely possible that the public impact of it is opaque, even to you. That can make writing a public impact statement feel like another box to check – an irritant more than an imperative. Maybe your study won’t directly affect the public or impact policy. But it will inform science going forward which will contribute to bigger changes that could well make a huge contribution to the well-being of the public. The public impact statement can be something that looks forward.
I think there was an excellent example of a well-crafted public impact statement in a recent journal article in CJEP. The article was published by MacMillan, Churchill, and Hourihan, and it’s entitled ‘Effects of valence and list composition on memory predictions, performance, and beliefs’. The abstract for the article assumes in the reader an understanding of terms like “metamnemonic”, “mixed-list design”, “pure-list design”, and “valence manipulation”. Another psychological researcher reading that abstract would absolutely understand those terms. (I assume – I don’t myself understand them well enough to say for sure.) This was the public impact statement that accompanied the article:
“Little is known about how emotions affect our sense of what we are likely to remember and what we are likely to forget. This study found that people believe that emotional words are more memorable than neutral words, especially when neutral and emotional words are studied together. Understanding the nature of this relationship can help improve the learning strategies we choose both in educational contexts and in daily life.”
That, in my estimation, is a very good public impact statement. I immediately understand what it is they did in the study, and I understand how the results can contribute to future research or inform a larger educational program in a small way. And I was able to glean that from one paragraph, without wading through definitions for metamnemonic valence manipulation.
When I write articles (like this one), I aim to create something at around a ninth-grade reading level. Not because I think that’s the level of the average reader – in fact, I believe that almost everyone reading this article is likely to have a greater competency than ninth grade. I do it because the easier it is to read something, the more people will be willing to read it. Why make people work harder than they need to, if your goal is accessibility? I bring this up because the way I determine this is a simple tool in Word that shows you your document’s reading level. I used that tool recently to review about 30 public impact statements from the CPA’s three journals, including CJEP. The average reading level was Grade 16. I don’t even know what grade that is. Fourth-year undergrad in psychology? First year Master’s? Some of them were so dense that the tool couldn’t even give me a reading.
Dr. Fernandes is right, and the intention is good. But it’s entirely possible that the impact statement is written from within psychology’s bubble. It may seem very straightforward to the researcher who is writing it, and to all of their colleagues. But not to the public. Not to journalists or writers or members of parliament or to me. A researcher publishing psychological research is presumably invested in the possibilities opened up by that work. The best opportunity for impact comes from visibility. And visibility without accessibility is pretty rare.
An example of what I mean is Dr. Fernandes herself. A wildly accomplished researcher, a journal editor, a respected star in the world of cognitive neuroscience, and a terrific science communicator. When I Google her name, the top result is the University of Waterloo, which stands to reason. The second is Google Scholar, also understandable. The third result is a podcast. (In fact, it’s the CPA podcast episode of Mind Full where Dr. Fernandes told us about her research into the connection between music and memory.) I thought it was likely that my algorithm was a little different than others, and made it more likely that the podcast would show up for me (after all, I go to that link quite often). I got a couple of friends to do the same Google search, and they got the same result.
In the communications world of social media, the central metric that matters to us when we collect data is “reach”. Yes, it matters how many people interact with our content, and click on the links we provide, and watch the videos we post. But what matters most is how many people have the opportunity to do any of those things – which means we have to reach them first. Most TV has more reach than most radio which has more reach than most newspapers which have more reach than most podcasts which have more reach than magazines which have more reach than social media. Your Bluesky or LinkedIn page has more reach than a journal article.
The way I see it, psychologists are one of very few groups who can reach inside the majority of those bubbles. And that means getting out there. In newspapers, magazines, blogs, podcasts.
Dr. Bruce Hutchison is an expert on emotional contagion, who has put his expertise out into the world via his Substack. That Substack currently has 39 subscribers. But every entry and essay he puts there is one more chance to be seen by more people.
Dr. Elena Antoniadis is not THE expert on memory. But she does teach about it. She puts some of her lessons up on her YouTube channel, and it was there that I discovered her video about memory. Her way of explaining it was simple, direct, and easy to understand, and I was delighted when she agreed to walk me through it for Psychology Month.
Madeline Springle also makes great use of YouTube, where she created a channel dedicated to her area of expertise as a Ph.D candidate at the University of Calgary. @MasterYourInterview has more than 60 videos about preparing for and nailing a job interview, and much of that content informed our article about job interviews – an article that also included THE expert (or maybe one of a very few who could claim the title) Dr. Nicolas Roulin.
In my role as communications specialist at the CPA, I run our various social media channels. More and more, I’m seeing psychologists speaking out about the issues that matter most. Racism, xenophobia, climate change, psychological regulation, domestic violence, healthcare, gambling, the opioid crisis, self-care, transphobia, fascism, corporal punishment, conversion therapy, the housing crisis, disinformation, AI, the importance of sleep, compassion fatigue, the questionable science behind Myers-Briggs, the benefits of light therapy, strategies to combat bullying in school, intergenerational trauma, the benefits of harm reduction strategies, the compounded trauma of refugees, workplace harassment…and so on.
They’re sharing their expertise at a time when it really matters. Sometimes it’s tentative. It’s understandable to be hesitant, especially in today’s environment where social media trolls and bots can make engagement unpleasant. It’s especially hard when you think that putting yourself out there risks judgement or criticism from your peers and colleagues in your profession. Dr. Jenn Vriend, a child psychologist in Ottawa, posted on LinkedIn about a recent decision in Ontario to change the standards for who can call themselves a psychologist. She put into words the sentiments of many:
“This process has been heavy, and at times honestly a little frightening to be part of.
What has stood out most to me is the courage and integrity of so many colleagues. Not loud. Not dramatic. Just steady, ethical, and deeply thoughtful.
I know how much fear can sit behind even a simple post or re-post. The hesitation. The second-guessing. The vulnerability hangover after speaking up.
And yet, people are still choosing to stand by their ethical responsibilities and their concern for the public. That has been incredibly grounding to witness. And, in many ways, it has helped me find my own steadiness too.
Quiet bravery is still bravery.
And there has been a lot of it.”
If not you, then who? If not now, then when? We are at time in our history that, prior to now, was relegated to…well, history. The rise of global authoritarianism, the rejuvenation of fascism, accelerating climate change, the mainstreaming of racism and homophobia, an increased threat from pandemics and formerly eradicated diseases, incel culture on the rise alongside femmephobia and toxic masculinity, the ripple effects of social isolation. There is a long list of threats to people around the world – and for the first time in many of our lives, those threats have not been relegated to distant parts of the world, but have come to our doorstep.
If psychology is equipped to understand why, it is equipped to understand how, and uniquely positioned to help others understand. We know how to build trust with the public. Let’s do that by appearing on their radios and TVs and podcasts and in their newspapers. CPA members can start with the Media Guide we created for this purpose. We know how to persuade individuals of objective truths. Let’s do that by persuading elected officials of the things we know to be true. CPA members can start with the Advocacy Toolkit created by Glenn Brimacombe, our Director of Public Policy. We know how people become convinced of falsehoods through disinformation. Let’s be a bulwark against that like Dr. Jonathan Stea, author of the book Mind The Science. We have significant expertise to share, and many of us do so in plain language to teach others about it through videos, or fact sheets.
I’m keenly aware of the somewhat circular logic of trying to write something in an effort to persuade psychologists to use their vast expertise to persuade others. What I am hoping to do is to make us all aware of the opportunity that lies before us, and the urgency of seizing that opportunity to centre psychology in as many areas as possible. That involves, in many ways, storytelling.
We can tell the stories of the people affected by wars and climate change. We can relay anecdotes about PTSD and bipolar disorder and toxic work environments. We can combat healthcare and mental health “wellness” grifters by walking people through the ways we arrive at data-supported and evidence-based treatments. We have the ability to help craft a narrative around our collective responses to antisemitism, gender diversity, conspiracy theories, or social isolation. When psychologists tell stories, they are telling the stories of people. And that, as we know (from psychology), connects with more people.
My job, as I see it, is to tell the stories of psychology. Psychology’s job, as I see it, is to tell the world the stories of its people.
Applying for a new job can be a nerve-wracking endeavour. Industrial/Organizational psychologist Dr. Nicolas Roulin from St. Mary’s University shares some insights into the process, illuminating the ways companies go about recruiting and the contributions of psychology to that exercise. Madeline Springle is a Ph.D. student at the University of Calgary, and she shares some tips for job-seekers about preparing for that important interview.
Most names in the following article have been lifted directly from the 1998 classic Office Space. The real people are Dr. Nicolas Roulin, a professor of Industrial/Organizational (I/O) psychology at Saint Mary’s University, and Madeline Springle, a job interview coach and a Ph.D candidate in I/O psychology at the University of Calgary.
Joanna was dissatisfied with her job. In just five months working there, she had realized how toxic the work environment was, and she realized that continuing to work there would have a detrimental effect on her mind and her soul. People were quitting all around her. Their work was being added to her own, without a raise in salary or so much as an acknowledgement of the increased workload. She knew she had to start exploring new opportunities.
Joanna updated her resumé and started looking on a series of employment sites. Although she felt that most anything would be better than her current workplace, she didn’t want to make the same mistake she had made when she accepted this current job. She was determined to find a company that was not only a good fit for her skills, but one where she could envision herself pursuing a career over the long term.
The first company whose job ad spoke to her was Initech, and they were right up her alley. They were asking for the database management skills she possessed, they were located a reasonable distance from her house, and they offered flexible office hours that would allow her to work from home whenever her kids were under the weather or her wife had to take the car to her own job. She wrote up a cover letter and sent off her application.
At Initech’s head office, HR manager Samir came in after the long weekend and checked his inbox. There were 209 messages, all from people applying for the open position! How on Earth was he going to get through all of these resumés on his own? Ah! He thought. I’m sure artificial intelligence can help here. He quickly pulled up a generative AI program, and plugged in the resumés of the company’s top-performing employees. He then had the program review all 209 resumés that had been sent in, and asked it to choose the top 10.
Although Samir wasn’t aware of it, the AI program had determined that two things, above all others, determined the quality of a Initech employee. Most of the top employees had included their middle names on their resumés. And many of them had been part of their high school bands. Joanna doesn’t play an instrument, and had not considered adding her middle name to anything. No one at Initech ever saw her resumé. Nobody contacted her to let her know they had received it.
Dr. Nicolas Roulin is an I/O psychology expert who was part of the team that conducted the search for the CPA’s new CEO, the team that chose Dr. Lisa Votta-Bleeker after Dr. Karen Cohen’s retirement. He says,
“AI has pros and cons, broadly speaking. If you use the right AI tools, it can make things faster, cheaper, and easier for an organization. In I/O psychology, recruitment often starts with a job analysis. The person in charge of the hiring will want to talk to the people who are currently doing the job, their supervisors, and maybe their subordinates. This is to figure out what exactly the job is about. What makes those employees effective, or less effective? What are the key issues they’re facing in that job? This might involve speaking with five, six, or even ten employees in order to get a good understanding. This can be quite time-consuming. If you use AI in an effective way, and understand how to implement it, you might be able to get similar results without having to speak with as many people.
The problem is that if you’re using the wrong AI, or the AI you’re using is built on very limited information or data, then you can get a situation where it tells you to look for three-named trombone players. If you have a very limited pool of data to train the AI, then it will do nothing more than replicate the biases that currently exist in that pool. If you are feeding in the data from all your employees, and most of them are middle-aged white men who play beer league hockey, then it’s likely your best performers are middle-aged white men who play beer league hockey. With a larger database, for example one of the large language models that are out there, running into a problem like this is a lot less likely.”
Joanna was ghosted by Initech, but she didn’t sit around to wait. She got right back to work and applied to a job with Initrode, which seemed to be looking for someone with her exact skill set. This job posting included a salary, and it was offering 25% more than she was currently earning. This time, she got a reply!
Initrode’s HR specialist Nina wanted Joanna to provide video answers to a series of questions. This next step was a one-way video interview, something Joanna had never heard of before. She was to record herself answering questions, looking at a camera, but there would be no interviewer there. How would you even go about preparing for that? Why would a company want that?
Madeline Springle is a job interview coach who hosts the Master Your Interview YouTube channel. She says companies do these kind of interviews because they mean every candidate gets the same questions, they all have the same amount of time to prepare and respond, and that this is a tactic that helps streamline the process when a company is conducting a high-volume hiring process.
“Companies likely understand how little candidates like these types of interviews, but they’re here to stay and there must be a reason. The purpose of the one-way video interview is to establish the first line of contact. It usually replaces the phone screening that was once the norm. The HR department would call the candidate to ask a series of screening questions and verify a few details. This would always happen during the work day. So would you rather have someone evaluating your video interview at a time when they’re feeling fresh and on their game, or call you when they’re at the end of a long day and this is the only time slot that could work for them?
The one-way video interview is really about deciding ‘should we move this candidate to the next round?’ You’ve submitted your resumé, then you get that video link. It’s a way to show you’re human, you can do the things you said you could do in your cover letter, and are you able to speak clearly about yourself.”
Dr. Roulin adds,
“One of the advantages of an asynchronous video interview is that the applicant can record their interview from any location, and at a time that’s convenient for them. If you have someone who already has a 9-to-5 job, they would previously have to take an afternoon off from that job to attend the interview. Now, they can record it at 10 pm if they like. That flexibility opens more doors to more people who might otherwise not have been able to do an interview in-person.”
Joanna had never talked directly to a camera to record something like this before. She made sure her background was clear, added a little wall hanging that really tied the room together, removed any distractions, and crafted her answers to the questions. She wrote them out and put them on a board just behind her camera, so she could read them and be sure her answers came out with the right wording. It felt robotic, but she guessed that was to be expected.
Nina sent her a kind, but brief email. Initrode had decided to go in a different direction.
Madeline says,
“There is such a fine line between extensively practicing and preparing, versus over-preparing and feeling like a robot when you deliver. In order to not sound overly rehearsed, try creating novelty in your response – something that will keep even you on your toes. At the core of this is adding variation to your interview response. The reason you’re feeling robotic is because you’re not emotionally connecting to your story. You’re saying the words, but you’re not actually present. You’re not actually experiencing it again as you share it. This is very common, especially when you’re feeling nervous. What you want to do is this – right before you answer the ‘tell me a time when you…’ question, jump back into that workplace environment. Think about how you felt at the time. Maybe it was five years ago. Who were you back then? Connecting to a former version of yourself will reconnect you to your story, and help you be less robotic and stiff when answering questions.”
Joanna was undaunted. She tried again, and after a while she received a response from a company called Chotchkie And Associates. Thankfully, they went with an initial phone interview for screening, and soon she was on her way to an in-person interview.
Chotchkie And Associate’s hiring manager Bob Porter was looking for a few specific things when he launched the search for their new Senior Database Administrator. Of course, familiarity with database management was essential. But he also wanted to find someone who would be adept at navigating issues that arose over the course of their employment. Specifically, he was thinking about a recent data breach in their customer files that had a catastrophic effect on the company.
Dr. Roulin says it’s quite common now for organizations to seek specific attributes and competencies in their hiring processes based on their own experience with how that role has been handled previously. They identify the most important aspects of the job, and determine what has allowed previous employees to excel there versus those who have been less successful.
“We often use what we call a ‘critical incidence technique’, where we try to identify specific issues that may arise in the role. We then try to understand what makes, say, Anne very effective at dealing with that critical situation, compared to Michael who is struggling to deal with that same situation. From that process we can try to recruit for the characteristics that fit best with the position.”
Bob Porter had determined what the company wanted in their ideal candidate, and prepared for a series of interviews that would be conducted over the course of two weeks. He brought in his colleague Bob Slydell, the manager who would be directly supervising the successful candidate. Some of the interviews would be conducted in-person, some over Zoom. Although Chotchkie & Associates used Teams internally for virtual meetings, Bob was aware that more applicants would be familiar with, and have access to, the Zoom platform.
As Joanna got in the elevator to head up for her interview, she went over some of her work stories in her head. She was nervous. What if they ask why I’m leaving my current job? Am I going to come across as disgruntled if I express how I am…disgruntled? Will I seem like a potentially disloyal employee if I complain about my current employment? And if I come up with a less abrasive version of why I’m leaving, won’t I be lying in my interview?
Madeline says focusing on red flags (your OWN red flags) is a very common mistake job applicants make when they begin an interview.
“Being focused on the negative – why they might not hire you, why they might not like your answer, isn’t helping you. Even worse, the interviewer can pick up on this negativity. Instead, make sure you focus on your ‘green flags’. Why you are qualified, what you bring to the job, and why you want this position. Your mindset going into an interview matters more than you think, so make sure yours is working for you, and not against you.”
Joanna put her doubts out of her head as best she could, and walked into her meeting with the Bobs confident in her ability to describe her past work experiences. It was all going well, and then Bob Slydell asked that dreaded question. “Why do you want to leave your current job?”
Dr. Roulin has studied the way we make impressions in situations like these. He says that while some of the research into making an impression is on the employer side, a lot more has been done on the side of the applicant.
“Some of the work I’ve done is on a topic called ‘impression management’, which has to do with how you can create a good impression in someone else’s mind. An applicant is asked questions, and their goal is to demonstrate that they have the experience and qualifications to perform the job. A good example of this is what we call the ‘STAR method’. For example, when you’re asked a question about an experience you had at work, you can build your answer based on a structure of the Situation, the Task, the Action, and the Result. If an applicant can tell their story with that structure, they can provide more information to the interviewer, and they can make a better impression.”
Joanna gathered herself, and answered. “I want to work somewhere where I can see myself having a career. When I saw your job posting, it looked like there would be good opportunities for advancement. I went on your LinkedIn feed and I saw that Chotchkie & Associates was celebrating Yom Kippur. It reminded me of a time when I was in college, working for the Student Association. There was a program in place that tried to promote inclusivity by adding elements of other religions to the usual celebrations of Christmas, Easter, or St. Patrick’s Day. It wasn’t really working, because it just jumbled up the event and no one really appreciated a nominal inclusion of other symbols in an event that was clearly not meant for them. I started attending celebrations outside the school, like Diwali, Eid, Nawruz. I learned a lot about those events, connected with people and even some of our students in those communities, and with their help I was able to collaborate with them to create specific, distinct events to celebrate their cultures. By the time I left school, many of those events were well-attended by students of all kinds, and I think it helped to build a sense of community. I got the sense that your company had that same sense of community, and that’s why I applied for this position.”
The Bobs looked at each other and nodded. Just the kind of flair they were hoping to see. Joanna got the job.
On this week’s Mind Full podcast we’re focused on one way psychology interacts with the healthcare system, specifically in the field of HIV and AIDS. Our guest, Dr. Sean Rourke, just won a major award for his life’s work, the inaugural Eric Jackman award from the Royal Society of Canada. From the days when an HIV diagnosis was seen as a death sentence to today, when early detection can result in a long and full life, he has been helping Canadians in a myriad of ways.
A diagnosis of cancer will affect each person who receives one a little differently. But it will affect everyone. Not just the person with the diagnosis, but the people around them. Family, friends, and co-workers need help as well. Psychologists can play a central role at every stage, from diagnosis to treatment to end-of-life care.
This week’s Mind Full podcast guests are friends. Bob Wakeham met Dr. Sheila Garland when he joined her study on insomnia in people who had been diagnosed with cancer. Bob shares his story and experiences with us, and tells us how Sheila’s involvement in his life made an enormous difference.
Remember the COVID-19 pandemic? It wasn’t that long ago, but many of us have kind of memory-holed the entire traumatic experience. That said, just because we don’t think about it any more doesn’t mean that the effects aren’t still being felt today. For example, rates of gender-based violence, including femicide, remain elevated above pre-pandemic levels. This is particularly the case in rural communities, and is evident in the attitudes and behaviours of kids in schools.
Canada legalized single-event sports betting in 2021. In the three years that followed, gambling on sporting events in the country rose tenfold. Today, one in five people who bet on sports do so every single day. Our young people are particularly vulnerable, and have been specifically affected by gambling addictions. Bruce Kidd and Steve Joordens are looking to ban advertising for sports gambling in Canada. Senator Marty Deacon has introduced bills to this effect. And Stanford psychologist Dr. Robert Sapolsky explains just what makes sports gambling so dangerous. All four joined us for this Psychology Month look at the dangers of sports gambling and the possible solutions to the problem.
In the early 60s, Bruce Kidd was preparing to represent Canada at the Olympics. He had just received the Lou Marsh award as Canada’s top athlete, and he was speaking at an event and being critical of the way gambling had infiltrated the sports world. At the head table of that event was Paul Hornung, the then-superstar halfback and kicker of the Green Bay Packers. Bruce remembers,
“[Hornung] passed along a note saying he’d like to meet me in the parking lot after the banquet, that being the traditional invitation to a fight, and I made a quick exit out the other way.”
Two weeks later, Hornung was suspended indefinitely by the NFL for gambling. He and Lions superstar Alex Karras had been betting on NFL games and “associating with undesirable persons” (gamblers). Both players were forthright and contrite, and the NFL felt comfortable allowing them back into the league the following year. Despite betting on NFL games, they were both elected to the Pro Football Hall of Fame in Canton.
Back then, gamblers were “undesirable persons”. They were the shady characters we imagine being played in a movie by Edward G. Robinson. To place a bet, you had to know where to find the illegal bookmaker, sneak in and out of their establishment, leave behind your money, and take your ticket to watch the game in a few days. It was a process. It also gave you time to anticipate your possible win when the Baltimore Colts covered the spread against the St. Louis Cardinals.
Today, things are much different. Handheld devices make it possible to bet not only up to kickoff, but on the distance of the return, whether the next play will be a running play, how many yards the backup tight end will have by the end of the first quarter. As that first quarter ends, you have TV commentators deviating from analysis of the play to analysis of the betting lines. They make suggestions for bets you might want to place before halftime. By the time the game is over, you might have placed eleven bets. You’re unlikely to have won all eleven.
The passion Dr. Bruce Kidd brought to the argument against sports gambling back in the 60s has not abated. Today, as a professor emeritus in Sport & Public Policy and a university Ombudsperson at the University of Toronto, he is doing everything he can to combat the dangers posed by the modern gambling landscape. He has created the website Ban Ads for Gambling to inform and energize the public to fight against the way sports gambling is marketed, in particular to teenagers.
Dr. Robert Sapolsky is a professor of biology, neurology, and neurosurgery at Stanford University. He agrees with Bruce that children are particularly vulnerable to gambling ads and apps.
“Children are absolutely more susceptible to this. We’ve got this very fancy part of the brain called the frontal cortex. It’s the most recently-evolved part of the human brain. We have more of it, and in a more complex way, than any other species. And what it does is things like self-regulation, impulse control, long-term planning, and executive function. The job of the frontal cortex is to calm the more emotive parts of your brain, like the dopamine system, or the parts having to do with aggression or sexual arousal. It tells those other brain areas ‘I wouldn’t do that if I were you. Trust me, I know it seems like a good idea right now, but don’t do it’.
The frontal cortex is the thing that keeps you from doing hideously impulsive things that seem like a good idea at the time, but that you will regret for the rest of your life. So why isn’t the frontal cortex keeping young people from making rash decisions? It’s because the frontal cortex is the last thing to develop. Most of your brain is fully developed around the time you’re getting toilet trained or learning how to walk up and down a flight of stairs. But the frontal cortex isn’t fully online until you’re about a quarter of a century old.
By contrast, the dopamine system is pretty much up-to-speed around the time you’re reaching puberty. This means a dopaminergic engine of disordered and distortive anticipation is there in you, while your frontal cortex is firing on only one cylinder. It can’t regulate it. It’s why adolescents behave in adolescent ways – impulsiveness, sensation-seeking, novelty-seeking, being slow to habituate to negative feedback, that’s what adolescence is about, and it’s mostly because your frontal cortex is still sort of percolating.”
It’s during that time of adolescence when young people, boys in particular, start paying more attention to both sports and their phones. When they watch a hockey game and between periods they see the play-by-play announcer and colour commentator debating what player will score the next goal, adolescents don’t have the same mechanism the rest of us do to slow down the impulse to place a bet based on the seemingly expert advice being dished out by the sportscaster.
Dr. Steve Joordens is a professor of psychology at the University of Toronto. He saw his old friend (and former boss) Bruce on TV, speaking as the Chair of the Campaign to Ban Ads for Gambling, and jumped on board immediately. For Steve, the most insidious thing about ads that encourage sports gambling is not just that they target young people, but that they use psychology to do so. The marketers, the app designers, and the promoters of gambling are all well-versed in methods of persuasion that are derived from psychological principles. Steve wrote an article about it, ‘Sports Gambling and the Weaponization of Psychology’, where he said,
“Society needs to restrict the marketing of sports gambling as soon as possible. It reflects a weaponization of psychology that is designed to create addictions. This is not hyperbole. A headline for The Hill reads ‘Sports betting has risen tenfold in three years. Addiction experts fear the next opioid crisis.’ A Harris Poll from November 2022 reported that 71% of those who bet on sports did so at least once a week with 20% betting once per day! The website suicide.ca has an entire page dedicated to helping those with gambling addictions.
Sports gambling is so dangerous because of the psychological power of random rewards. When players gamble, they lose more often than they win, However, the random nature of wins means they never know when that next win is coming. They start chasing that next win. At the neuroscientific level, the hormone dopamine is released when one is chasing a desired outcome and this release feels good, literally the thrill of the chase. Each loss can make the player feel one step closer to that next win, which always feels like it’s just around the corner. This makes the player ‘resistant to extinction’. Once they start, they don’t want to stop, especially after a string of losses.”
Dr. Sapolsky describes the mechanism by which dopamine encourages certain behaviours. Dopamine is the neurotransmitter that regulates pleasure, and many of us are familiar with dopamine experiments done with animals like rats or monkeys. For example – a light goes on, which is the signal to press a lever, and that pressing of the lever distributes a treat of some kind. But the dopamine isn’t released when the treat is revealed, or when it is consumed. And it isn’t triggered when the lever is pressed. Instead, the dopamine rush felt by a rat or a monkey or indeed a human being happens when the light comes on. It’s the anticipation of the reward, not the reward itself, that activates our pleasure centres. He explains further.
“Dopamine goes up when the signal comes on. You see the light and you think ‘oh, this is going to be great – I press the lever ten times and I get my reward. I have control, I have agency!’ The dopamine is triggered by the anticipation, not by the reward itself. And if you block the dopamine release, you don’t get the lever-pressing. Because it’s not just about the anticipation, it’s about the motivation you must have to do the work needed to get that reward.
For those familiar with our U.S. Constitution, it’s not the ‘pursuit of happiness’, it’s the happiness you derive from the pursuit, and the motivation you derive from the pursuit. We’re a totally bizarre species in that a monkey can learn to lever-press, raise dopamine with the anticipation, and get a reward thirty seconds later. While we’re the species that can get a signal, and do the required work, and wait for a reward years from now. To get a good job because you studied hard in school, or to leave the planet better for your grandkids, to get a reward after you’re dead! We can sustain that anticipatory dopamine and work really really hard for rewards that are way off in the future.
Where this applies to gambling is if we take the scenario of doing the work and getting the reward, and we shift things a little. This was the work of a guy named Wolfram Schultz at Cambridge, who’s the pioneer in this field. We shift things so you get the signal, you do the work, and you get the reward – only 50% of the time. So what happens to the amount of dopamine you get when the signal comes on? Is it a little bit smaller than when there’s a 100% chance of a reward? No! What you see is that dopamine goes even higher, and 50% drives the system even more. You’ve now introduced a new word into the experiment – ‘maybe’. And ‘maybe’ fuels the system like you wouldn’t believe.”
50% is, in fact, the magic number here. At 40%, the dopamine is not as strong, because the person knows that they are more likely than not to be disappointed. At 60%, the same thing happens because the person knows they are more likely to get a reward than not. 50% creates the greatest uncertainty, and therefore the greatest dopamine rush. This is a psychological principle that has been central to casinos around the world. Blackjack players win about 49% of the time. Craps, 49.5%. Roulette, 48.6%. Not only do the almost-even odds enhance the anticipation of the players, this setup keeps them at the table playing longer and spending more money.
Gambling scandals are nothing new to sports. Boxing has been dealing with accusations of match-fixing since the beginning. There have been scandals in sumo wrestling, badminton, darts, and e-sports. But in North America, the biggest gambling scandals that stick in the public consciousness have been around baseball. The National League was established in 1876 to provide an alternative to the wildly corrupt match-fixing culture that permeated the sport at the time. Eight members of the 1919 White Sox conspired to throw the World Series at the behest of gamblers. Pete Rose was famously banned for life in 1989 because he bet on his own games. In the early 80s, Major League Baseball threatened two of the sport’s biggest icons, Willie Mays and Mickey Mantle, with permanent bans because they were working as greeters at a casino. Baseball spent more than a century fighting to preserve the public perception of integrity in the game, and any association with gambling undermined that credibility.
Then, in 2018, the U.S. Supreme Court declared a federal ban on sports gambling to be unconstitutional, and the floodgates opened overnight. Gambling could now expand outside Nevada, where it had been confined to Las Vegas for decades. Sports books, apps, and website sprang up almost immediately, and the money began pouring in. By 2021, the Canadian government had followed suit, legalizing single-game betting in our country.
It’s hard, one imagines, to say “no” to money. Especially when that money comes in really, really easily. Every major North American sports league has hopped into bed with gamblers with both feet. Even baseball, which for so long had fought to keep even the appearance of impropriety at bay, caved to the allure of the easy dollars. Why try to track down and make deals with sponsors and advertisers when gambling apps just deliver a dump truck full of money to you? It requires little effort to say ‘yes’, and your sport is now suddenly more lucrative than ever.
The sports leagues are raking in easy money. Athletes are raking in easy money. Connor McDavid and Wayne Gretzky are teaming up for Bet MGM ads. The Manning brothers are shilling for Caesar’s Sportsbook. Charles Barkley is endorsing FanDuel, LeBron James is endorsing DraftKings, and even college athletes like gymnast Livvy Dunne are appearing in ads for Fanatics Sportsbook.
It takes a huge amount of money to pay all the celebrity endorsers, to run ads from beginning to the end of every game, and to sponsor every halftime show, every intermission, and every pre- and post-game show we sports fans consume. That money comes from people. People who are gambling on sports, who are getting in over their heads, and who are increasingly seeing gambling as a normal, obvious part of the sports-watching experience.
Is it possible to put this cat back in the bag, to convince sports leagues swimming in easy money to go back to their now-antiquated business models? In just a few short years, the intertwining of professional sports and legalized gambling has made such a task gargantuan. Steve and Bruce think the place to start is with the advertising, and they are doing everything they can to stem the tide. Steve has hosted webinars, written op-eds and essays, and in 2025 he appeared before the Senate of Canada on behalf of the CPA. In his testimony, he said,
“Allowing any form of marketing of gambling runs completely against our members’ attempts to prevent and address mental health issues. It pushes all Canadians to consider betting, with an especially strong impact on our children and our marginalized communities. There is no need to market gambling. Would-be gamblers can easily find legal gambling on their phone apps, apps which can be policed. The Canadian government must not allow companies to push our population into addiction and, with all due respect, I ask all of you to help us help Canadians. As a country we can do better. We should and must ban the marketing of gambling.”
The Honorable Senator Marty Deacon was one of those who were receptive to Steve’s call to action. She says she doesn’t (yet) regret her vote in 2021 to legalize single-sport betting, but acknowledges that more care should have been taken at that time in regard to the advertising component of legalized gambling.
“Without the regulation of gambling, it was all happening in an underground, unregulated way, and taking in billions and billions of dollars. I don’t regret voting for the bill – yet – but the part that probably wasn’t given enough time and consideration was the media piece, the advertising piece. When the bill became law in the summer of 2021, a door opened quickly and strongly to advertise, and that was out of control. Part of our inundation of advertising is due to the way it was set up. Private sector companies were allowed to operate and compete against one another, which drove up the amount of advertising.”
Senator Deacon has recently introduced a bill to limit the advertising of sports gambling. What the bill says is that ads for gambling would be prohibited during the airing of the game itself. From puck drop to final whistle, from opening pitch to final out, there would be no gambling ads encouraging us to bet our money. (In fact, she is re-introducing this bill, which has moved through the Senate and the House before but has been stalled by elections and new governments. When a federal election chooses a new government – even if the incumbent party is victorious – all bills that have not yet become law die. They must then be re-introduced and go through the same procedure all over again.)
“I’m passionate about sport, and safe sport for all. What was amazing to me was the impact this was having globally on certain populations. For older people, just an annoyance with constant ads on the TV and pop-ups on their phones. But a combination of electronic communication, the pandemic, and traditional media, has left young people really exposed. And the ones who seem to be most impacted by addictive behaviour are younger males, around 14-34. All populations are vulnerable, but that’s a significant one.”
In just the past two years, the number of gambling scandals affecting the sports world in North America has skyrocketed. College sports have had to deal with a litany of incidents where players and coaches are found to be gambling. The NFL has suspended more than a dozen players and team employees. Golf, tennis, UFC, the NBA, and the NHL have all had issues of their own. And in baseball, the scandals are piling up in a major way. Shohei Ohtani’s translator stole more than $16 million to fund a gambling habit. Other players have received lifetime bans and even umpires have been disciplined for gambling. It’s a sport that lends itself remarkably well to today’s gambling landscape. When you can bet on the first pitch to the second batter in the fifth inning being high and outside, then what seems like a meaningless one-off play in the game can be an alluring prospect for that pitcher.
When the lines that hitherto defined the integrity of a sport become blurred, it sends incredibly mixed messages to the players involved in that sport. Players who, in many cases, are young enough that they do not yet have fully developed frontal cortexes either. You can give an interview on the DraftKings pregame show, you can accept a boatload of cash to endorse FanDuel, but you’d better not actually gamble! THAT’s unethical!
When the lines get blurred for athletes, they must also get really blurry for fans. Where once you might have rooted for the Ottawa RedBlacks on TV 18 times per year, and maybe attended a couple of games, now that doesn’t feel like being a committed fan. If you’re truly committed to the RedBlacks, you’ll bet on them to win, to cover the spread, and for Adarius Pickett to break up two passes in the third quarter. It’s just what people who watch sports do, isn’t it? Dr. Sapolsky says the ability to make these in-game decisions is particularly difficult to manage, because it doesn’t give the frontal cortex time to catch up.
“When you’re sitting in your Vegas hotel room late at night and thinking ‘oh my god, there goes half the kids’ college money’, it gives you some time to think about it, and some time for the frontal cortex to get things under control. By contrast, when it’s a fast decision, it is hopeless that the frontal cortex is going to get there in time. It’s the impulsiveness of violence, or the impulsiveness of pressing a button on your phone.
When I was a kid in New York City, they legalized what they called ‘off-track betting’, where you no longer had to go to the racetrack itself to place a bet. They had these nice shiny locations with friendly high school kids behind the counter taking your money, and it was all straightforward. And best of all, the money the state was getting from off-track betting was being spent on education. Great news right, it’s being used for something beneficial! What gets lost in that is that the money you are taking from people who are gambling away their savings is disproportionately from poor people. It’s redistributing the wealth in the worst possible directions. Here in the United States, a lot of that is because people without money are psychologically manipulated into thinking ‘I’m actually a rich person who just hasn’t gotten rich yet’.”
A gambling addiction is a little bit different than other addictions, in that the effects of it can be much more devastating. Once a person realizes they need help for a dependence on cocaine, or alcohol, they can take the steps they need to get better. Although it can be very difficult, with the support of family and friends they can turn things around and recover. With gambling, the same is true – but even after recovery there is something hanging over their head. An enormous and often life-altering amount of debt. It’s no wonder that suicide prevention websites have sections dedicated entirely to gambling.
So what can we do? Most people – including many mental health professionals – think that an outright ban on gambling is a non-starter at this point, and that even attempts to ban advertising for it will face stiff opposition. The proposed solutions nibble around the edges, and could make a difference, but they are unlikely to do anything major to stem the tide. Steve has a few suggestions, including adding a feature to gambling apps where every time you log in you get to see a running count of how much money you have won or lost. It might make us pause for a moment when we open our app and see that we’ve lost $12,000 in nine months. That pause might give our frontal cortex enough time, and enough data, to make us reconsider going back in to place another bet and lose more money. He also makes a point about the way we advertise (or don’t) other products.
“We have legal THC in Canada, you can go buy cannabis anywhere you want, but it is not advertised. Remember the Steppenwolf song The Pusher from the 60s? It makes the distinction between someone who goes out and finds a dealer, versus someone who isn’t looking but the dealer finds them and pushes their product. A ban on advertising for THC says ‘it’s a free country, you can do what you want to do, but there’s a reason to worry here so we’re not going to encourage this behaviour’.”
Dr. Sapolsky says that while the intention makes sense, an outright ban on gambling itself could end up backfiring, particularly among young people.
“I can see [making it illegal to gamble] backfiring, with the allure of the illicit. I’m not sure it would work on young people, because the ban could make them feel like teenage desperados, you know. Cigarette companies have figured this out, introducing vapes in bright colours and with exotic flavours. It combines the appeal of the illicit with the attention-grabbing novelty of the product, and even though vapes aren’t advertised, the industry is incredibly lucrative and really skilled at taking money from teenagers.”
Senator Deacon says we’re going to get there one step at a time.
“To move this through the Senate and the House, based on what we’ve learned with alcohol and tobacco, I felt that a full ban [on advertising] would have really slowed down the intent of the legislation. My bill is a moderate way to get the ball rolling, and the House can take over the bill and do a full ban if that’s what they like. Some of the things we could be looking at are ‘ten before and ten after the whistle’ (so no ads during the game itself). Denmark is doing this, and gambling companies there can advertise only between 1 am or 5 am. Also, anyone doing the advertising, or appearing in the ads, must be over 25 and can’t be an athlete.”
She also says that while letters and emails to MPs do work, emails and letters to senators do as well. For people who care about this issue and are passionate about it, contacting your elected officials, and unelected officials, goes a long way and could move legislation along to the point of a full ban.
“Now the bill is sitting in the House, and it has been presented there. We want families, organizations, and Canadians to reach out to their MPs. Bruce’s Ban Ads For Gambling group is very effective in doing this, and it makes more of an impact coming from him and from Steve than it does coming from me.”
Bruce, and Steve, and their colleagues from all over are going to continue this work as long as they can. As Dr. Sapolsky said, we human beings are unique in that we can put in the work today for a reward that may not come for a long time. To join the campaign, visit Bruce’s website and click ‘get involved’ for a form to send a letter to your MP. Be vocal about your opposition to sports gambling ads. And if you’re on one of those apps, take a moment to look back over your results and take stock. Maybe determine whether it’s a good idea to continue placing those bets. Your frontal cortex will thank you.
Just about every little kid has accidents from time to time. But more than one poop accident in a month (encopresis) or more than two pee accidents per week (enuresis) might be cause for concern. Dr. Jen Theule helps explain what signs to look for, how best to potty-train kids, and how psychologists help resolve problems that might occur as children get a little bit older.
How do we gather information to store it in our memories? How do we retrieve that information when we need it? And can you actually forget how to ride a bike? Dr. Elena Antoniadis, psychology professor at Red Deer Polytechnic and an adjunct professor at the University of Calgary, joins us for a look at how we form memories, how we can enhance our recollection abilities, and more.
Zaineb Bouhlal, the CPA’s Membership Database and Services Administrator, says she has forgotten how to ride a bike. Is such a thing possible? After all, it’s the most-clichéd thing we’re all supposed to remember as long as we live. “Like riding a bike” is the phrase used to describe most everything we store in our procedural memory. Biking, swimming, typing, driving a car, any skill that involves sensory-motor coordination that we’ve practiced and acquired is one we can re-gain if we’re put back into that same setting.
Dr. Elena Antoniadis is a psychology professor at Red Deer Polytechnic and an adjunct professor at the University of Calgary. She says,
“Once you’ve learned to drive a car it would be very difficult to forget how to carry out all the operations that go into driving a car. But it’s not a memory that our conscious or declarative systems have access to. So, for example, we can’t tell a younger sibling how to ride a bike – it’s not something we can write a manual for. It’s something that the body registers, and then the implicit memory system builds the memory of that skill.”
There are memories that are encoded explicitly – like facts, knowledge, the things you learn in school. You are making a conscious decision to remember those things, and what makes a memory “explicit” is that we can consciously access it and describe its contents, rather than simply showing it through behaviour. Then there are memories that are encoded implicitly – this is how we build habits, conditioned reflexes, and learned responses. The brain registers patterns without us being aware of them. The basal ganglia in the brain helps us build the skills, the habits, and the automatic responses that come from the implicit encoding of memories. Language is often one of those areas that we learn implicitly from a young age.
Before I worked at the CPA, I worked at The Dementia Society of Ottawa & Renfrew County (DSORC). DSORC runs programs for people living with dementia, programs which often make use of deeply encoded memories to recall songs from childhood, or to move and exercise in familiar ways. When I was there we had an Arabic-language program, for people who had grown up in the Middle East but now lived in the Ottawa area. One older man came to that program with his family. They had come to Canada from Saudi Arabia a decade prior, and now their father was living with dementia. Unfortunately, the program wasn’t working very well for him because, although he had spoken Arabic with his family for his entire life, he no longer spoke the language. Instead, he was speaking a language they had never heard before. After a while, the Dementia Care Coaches determined that he was speaking Farsi. He had grown up in Iran, but had never told anyone in his family about his childhood in another country. Now that he was losing his short-term memory, and his longer-term memory was starting to fragment, he was left only with those memories that had been deeply and implicitly encoded in him some 75 years ago.
By contrast, memories that have been explicitly encoded behave differently. We use different methods to retrieve them, and our methods change over time as we experience more of the world from a personal perspective. Says Dr. Antoniadis,
“Children are more emotionally attuned to those around them, their environment, and their primary caregivers. They rely more on the emotional parts of the experience to build their memories. As we age we can rely more on our own lived experiences, the episodes that take place in our lives. I witness this in my own classes. I see mature students who are returning to school, and they can connect something factual with something they’ve experienced in the workplace or in a familial environment. Because they have a broader repertoire of meaningful experiences they can connect with the information they’re receiving.”
That increase in experiences can be a little bit of a double-edged sword when it comes to memory. Think of major events that happened in your life, and the way you remember them now. For me, a good example is 9/11. I know I was in radio school, and that I was with Vicky McKenzie. But when I discuss that moment with Vicky today, we have very different recollections of how we responded, who was around, and what we did next. Either one of us is right and the other wrong or, more likely, we’re both a little bit wrong.
A major event like that one feels like it happens in an instant, and that we have a snapshot in our minds that will be accurate forever. But it doesn’t really happen in an instant. After the event, there is news coverage of it. Your family is going to be talking about it, your co-workers or fellow students or schoolyard friends will also be talking about it. Now, within a few months of the event, you have added untold amounts of information to that first memory, which can distort your recollection of the specific facts.
I am almost certain that we watched, in real time, the second plane hit the World Trade Centre. Vicky says we started watching only after that happened. I remember going, later that afternoon, to donate blood with Jamie Johnston. Partly because we didn’t really know what else to do, and partly to put on our journalist hats to talk to people who were also doing the only thing they could think of in that moment. Jamie tells me we actually did that several days later. Dr. Antoniadis says this is quite common.
“Many times we have factual information about an occurrence. That information comes in separate from the memory itself, but becomes integrated into the memory. This is the reason why sometimes police officers who arrive at an accident or something like that will separate witnesses to make sure their stories don’t impact the other person’s recollection. Hearing another witness describe what they saw can become integrated into our own memory of the event, even one that happened moments earlier.”
In 1994, Chuck Knoblauch of the Minnesota Twins finished the major league baseball season with 45 doubles. That season was shortened by a strike that resulted in no World Series being played, much to the chagrin of Expos fans who thought they had a great chance at their first title, and Blue Jays fans who were denied a chance at a three-peat. Had the season lasted a full 162 games, Knoblauch was on pace to hit 65 doubles and threaten the all-time record of 67 set by Earl Webb in 1931 with the Red Sox.
This is a fact I know. It’s one that has stuck in my brain since my youth, and while there’s no good reason for me to remember, I have never forgotten what might have been in 1994. I find it somewhat interesting. My wife finds it somewhat irritating. “You can remember how many doubles Chuck Knoblauch hit in 1994, but can’t remember that you were supposed to take the garbage out?” she’ll say. And I will respond with “I dunno – that’s just how my brain works, I guess”.
It turns out though, that this is how all of our brains work! Our capacity for short-term memory is finite, but our long-term memory retention is – as far as we know – limitless. Dr. Antoniadis explains more.
“Short-term memory has limited space, but long-term memory is limitless in its storage capacity. We have variety in the mental operations we perform – encoding, storage, and retrieval. But we also have variety in the types of information that we create. Long-term memory is, according to the scientific literature, limitless. We can continuously keep learning and acquiring new information.”
Dr. Antoniadis says that because our short-term memory has a finite capacity, there can be a bottleneck where we are subconsciously deciding whether to commit information to more long-term retention, and deciding what ideas we might discard. I likely won’t need to remember, ten years from now, that I took out the garbage today or shoveled the driveway. It won’t come up in pub trivia. But Shohei Ohtani’s 3-homer 10-strikeout playoff game…that might come up! It’s going in the vault.
So, I’ll remember that for pub trivia purposes, and it may or may not come in handy a decade from now. But what of the people who excel at that kind of memory retrieval? The people like Ken Jennings, Mattea Roach, or Amy Schneider who can get on Jeopardy! and just crush it?
“Retrieval depends heavily on cues and context. Individuals who are practicing retrieval and recollection of accurate information may be using retrieval cues that will help them enhance that. Can they use something about where they were at the time they learned it? What they were doing when it happened? They’re focused on matching the cues that were present when that information was presented. This happens in school too – if you’re writing an exam in the classroom where you learned the information, you’re more likely to be able to retrieve that information than you would be if you wrote it in a different classroom.”
So…does that mean that the old adage is true? The one that says if you study under the influence of weed or alcohol you should write the exam in the same state so you can maintain the same frame of mind and to increase the likelihood that certain cues will assist you in retrieving the information you need? Dr. Antoniadis says yes.
“The concept is supported research findings. It’s called ‘state-dependent memory’. When we’re in a certain state – an emotional state for instance – we’re more likely to retrieve memories from that state. When we’re happy, we retrieve joyous memories. When we’re sad, we’re more likely to recollect sad memories. When our physiological or emotional state matches experiences we’ve had with a similar state, we’re more likely to retrieve the memories from that time.”
We hear a lot about scent and memory in popular culture. Perhaps more than any of our other senses, smell triggers memory cues in subtle ways that make it easier for us to recall old events or retrieve information buried deeply in our minds. Dr. Antoniadis says this is because our olfactory sense (smell) is very much connected with the parts of the brain that houses the instinctual parts of our memories.
“Instead of it being something we are consciously aware of, or something we can explain or articulate, it’s a non-declarative memory. That means it’s something we feel, something we can enact or show through our behaviour, without being able to explain it. We might have an emotional reaction to a frightening cue without being able to explain why we responded that way. Other times, emotional reactions can be the impetus to conjure up the conscious memory if it’s there. It can be a gateway to a conscious recollection of a specific memory.”
A lot of memory exists in a place beyond our specific awareness. When we say we can’t remember something, that doesn’t necessarily mean we haven’t stored the memory, but that we’re having trouble retrieving it. Like thinking we have forgotten how to ride a bike, when in fact we might well remember exactly how to do so when we’re put in a situation that is reminiscent of the time when we did ride a bicycle all the time.
At the CPA, we are going to put this to the test. It will be an anecdotal study, and the data will be applicable only to Zaineb. Once the snow has melted, in late May or early June, and Stewart starts riding his very expensive bike in to work again, we are going to perform an experiment in our parking lot to see if Zaineb can, in fact, summon the bike-riding knowledge she once had when put in that situation. It will be one more experience that we can all add to our repertoire of experiences that allow us to draw on our memories.
Stewart’s bike is very nice, and he takes tremendous care of it. We will wait until the day we conduct the experiment to tell him that his bicycle has been volunteered. So don’t tell him before then.

Liisa Galea
Dr. Liisa Galea is a scientific lead for the CAMH (the Centre for Addiction and Mental Health) program womenmind™. It’s a community of philanthropists, thought leaders and scientists dedicated to tackling gender disparities in science, and to put the unique needs and experiences of women at the forefront of mental health research.
Womenmind™ Liisa Galea
“You know how to *take* the reservation, you just don't know how to *hold* the reservation. And that's really the most important part of the reservation: the *holding*.”
- Seinfeld, ‘The Alternate Side’, 1991
The National Institute of Health (NIH) in the US introduced a policy* in 1993 where applications for research that plans to involve human subjects for clinical trials must address the inclusion of women, minorities, and children in the proposed research. As a result, the scientists applying for research grants did exactly that. They included women, minorities, and children in their studies. But to what end?
It’s easy to include women, minorities, gender diverse people, but if you don’t look to see if it’s affecting outcomes for those individuals differently, then you’re doing only half of the work – and missing the part that makes inclusion important. But precious little research, since the introduction of that policy, has made that distinction.
*It should be noted that it is quite difficult, at the moment, to ascertain exactly when the NIH instituted that policy, or what the outcomes have been, since the new American presidential administration has scrubbed their websites and resources of any language involving “minorities”, “disparity”, “bias”, and even “women”.
Dr. Liisa Galea leads the Women’s Health Research Cluster at the Centre for Addiction and Mental Health (CAMH) in Toronto. She is the principal editor of Frontiers in Neuroendocrinology, the Past President of the Organization for the Study of Sex Differences and co-Vice-President of the Canadian Organization for Gender and Sex Research. She is also the scientific lead for the CAMH initiative womenmind™ and a Seinfeld fan.
“I grew up in a time when I had to wear a skirt in school because I was a girl. I’m so grateful to my parents for saying I was smart and could do anything I wanted to do…except perhaps become Pope! I was told I was different because I was a girl, but it didn’t upset me – it just made me curious as to why people thought that. When I started university, I got really interested in the area of female brains vs male brains and I wanted to know all about the differences and what that might mean for our health.”
womenmind™ is a community of philanthropists, thought leaders and scientists dedicated to tackling gender disparities in science, and to put the unique needs and experiences of women at the forefront of mental health research. Dr. Galea and Dr. Daisy Singla, a clinical psychologist who specializes in perinatal mental health, are womenmind™ scientists who do a lot of this important work.
The gender disparities in healthcare are real, and they are significant – particularly in the area of mental health. Diagnoses of mental health issues can take up to two years longer for women compared to men. There is a sense in the public sphere that men don’t talk about their feelings as much as women do, and are less likely to seek help with psychological issues. Despite this, just looking at mental health disorders, there is still a delay in diagnosis of more than two years for women. That delay can interfere with treatment plans – if you’re being misdiagnosed or dismissed with your symptoms you’re not getting the treatment you need, and we all know that earlier interventions lead to better outcomes.
A study done by the World Economic Forum showed that globally, women spend 25% more of their lives in poor health than men do. Dr. Galea thinks this is partly due to health science being historically dominated by men studying males.
“In terms of mental health specifically, there are many reasons for the delays in diagnosis, but one of the major reasons I think is because most of our medical knowledge – including the symptoms on checklists for diagnoses – are based on the experiences of men. So much so, that we often call symptoms for mental health disorders in females ‘atypical’. We use ‘atypical’ a lot in the context of neurodiversity – autism, ADHD, and so on. And there are more males diagnosed with those conditions. We see more females than males diagnosed with depression, but we also see that ‘atypical’ label applied to depression in women. If there are twice as many women diagnosed with depression as men, how are their symptoms ‘atypical’? I think it’s because our scales were developed a long time ago, thinking about findings in males and the experiences of men.”
As a result, healthcare providers don’t acquire enough knowledge about sex and gender disparities in disease presentation and symptoms. This has real consequences for women in the healthcare system, but also for funding bodies. As a researcher that’s been in this field for 28 years, Dr. Galea gets a lot of comments from editors and funding agencies that *this [female-centric subject]* isn’t a really important thing to study because it’s “only in a subset of the population”.
Dr. Galea and her team did a review, looking only at male/female studies in neuroscience and psychiatry. 68% of studies were using both male and female participants, but only 5% of those studies looked to see whether sex made a difference. As Dr. Galea says, “you can have 2 females and 8 males in your control group, but the reverse in the treatment group, and you can’t do the analysis properly because you don’t really have the sample size to see if it made a difference.”
27% of the studies were focused solely on males, and 3% solely on females. Dr. Galea’s team then looked at Canadian grants, which resulted in similar percentages. In 2023, mental health specifically for women made up less than 1% of the funding of the Canadian Institutes for Health Research (CIHR), the major federal agency responsible for funding health and medical research in Canada.
Funding for research is, sadly, a hot-button issue at the moment as the new American government tries to shut down funding at the NIH for everything they deem to be “woke”. This has impacted many of Dr. Galea’s colleagues and the work they do, especially since the cuts seem to have been attempted in the most damaging and misguided way possible. The new administration looked for the key words they didn’t like, and cut funding for everything that contained words like “bias” or “diversity” or “environmental”. They also targeted words like “trans”, “non-binary”, “female”, and “woman”.
This could result in the ending of studies into things like the gut microbiome, where one of the measures is alpha-diversity and beta-diversity – referring to the variety of bacteria that live in one’s gut. Electricity studies using vacuum tubes which require a current called “bias”. And studies involving women’s health. Dr. Galea says this is even more dangerous than it seems, because stopping the study of women’s health affects men as well. She gives an example,
“Lazaroids were a drug that was discovered for stroke recovery. It worked miracles for people who had suffered strokes. It was discovered pre-clinically first, where it worked on mice and rats, and then it went to double-blind randomized control clinical trials, our gold standard. It turns out most of the pre-clinical work was done in males. The early clinical trial was done all in men as well, since men are more likely to suffer a stroke earlier in life (but this switches to more women later on in life). It failed phase 3 clinical trials, which included women, and the drug is not on the market. It put the drug company out of business. But when people did secondary analyses, it turns out lazaroids work wonders in men – but not in women. In fact, in women it might have made things worse. But that’s a drug that’s now not on the market that might do wonders for men’s health! Isn’t it in our collective interest to find out what drugs work better in different populations?”
This upheaval could have devastating consequences for the future of women’s health, an area that has critical problems already. Consider menopause. This is something that will happen to 50% of the population. And yet, 0.5 % of all studies in neuroscience, and in the field of brain health in general, are on menopause. Physicians get about 1-3 hours of training on menopause and its effects on health.
When women go through menopause and have significant problems, they get sent to specialists – gynecologists. But – only 30% of American gynecological programs had anything about menopause in them. So well above half the time women get sent to see specialists for this, they’re going to see someone who hasn’t been trained in it, and may have learned very little about it. Says Dr. Galea,
“We have to become our own specialists, but we need informed research to know what we can do to offset our symptoms. Laura Gravelsin (one of my postdocs) and I just had a paper accepted called ‘One Size Does Not Fit All: Type of Menopause and Hormone Therapy Differentially Influence Brain Health’, because there are many hormone therapies and many menopauses, and we have to determine which one works for us individually.”
Not all scientists who study women’s issues are women, and not all women specialize in those issues. But having more girls going into scientific disciplines, and being supported along the way, can’t hurt. This is another of womenmind™’s goals. Dr. Galea points to the fact that there are more female psychologists, and physicians, than there are male. And yet, at the dean level, or director or supervisor level, the proportion of women steadily decreases the higher in rank you go, compared to men. She says,
“Girls are very interested in all scientific fields at a very early age, but as time goes on and we get further and further in our career, the disparity starts to grow. At the university level, you see more women and girls in the sciences, but the gap gets a little wider the further up you go, at the graduate level and then at the assistant professor level.”
With this in mind, womenmind™ has a robust mentorship program for all female and gender-diverse scientists that has seen remarkable results. About 60% of the female and gender-diverse scientists at CAMH have gone through the mentorship program, and there is a staggering 100% approval rate – every single person coming out of the mentorship program has said they would recommend it and they want it to continue.
And continue they will, with the passion and determination of the new scientists and the veterans like Dr. Galea. In addition to womenmind™, she runs her own lab investigating how hormones (mostly estrogens) influence the brain. They focus on stress-related psychiatric disorders like depression, and also Alzheimer's. Dr. Galea also runs the Women’s Health Research Cluster which in the realm of knowledge translation, and seems like a lot of fun! They just had an event in Toronto called ‘Galentine’s Day: Love your Brain’ which was about girls and women and anyone who identified as such loving their brains through hormonal changes like puberty and menopause.
The experiences of women and girls going through hormonal changes are varied and diverse. The path through adolescence, or menopause, is rarely a straight line. Nothing in life is a straight line! Even Dr. Galea’s journey to doing the work she does today (and Parks and Rec fandom) took numerous twists and turns. She says,
“I started in engineering first, and took Psychology 101 with Susan Lederman. She works in perception. She said ‘I’m the first Canadian, the first woman, and the first psychologist to be asked on a NASA panel’. She was there because astronauts were complaining they couldn’t feel anything through their gloves when they were out on a spacewalk. I was hooked. I thought, ‘that’s so interesting, I want to learn that’. It’s not at all what I ended up doing, but I took a lot more psychology as a result. I ended up studying women’s brains, and I’m always going to do it!”
Someone’s got to do it. And someone else entirely has to support them by making it a priority to ensure they continue to get to do it. With initiatives like womenmind™, the Women’s Health Research Cluster, and the research being done by Dr. Galea and her colleagues, the future of gender-inclusive health science looks promising. But if we want to make the most of that promise, the scientific community and policymakers must make it a priority to ensure this research continues.

Madeline Springle is a second-year Ph.D. student at the University of Calgary, who is winning awards for her ability to mobilize knowledge. Specifically, she is taking the research she has done into one-way video interviews, and using it to help people who might use this knowledge to better prepare for their own job search.
As we close out Psychology Month, we wanted to highlight knowledge translation (explaining the science for a more general audience) and knowledge mobilization (putting new findings into practice such that they help those they were designed to help) because without those, science exists in a vacuum!

Cette semaine, dans le cadre du Mois de la psychologie dont le thème, cette année, est « Les femmes et la science », nous présentons Sophie Bergeron, Ph. D., qui détient une Chaire de recherche du Canada sur les relations intimes et le bien-être sexuel au Département de psychologie de l’Université de Montréal, où elle dirige également le Centre de recherche interdisciplinaire sur les problèmes conjugaux et les agressions sexuelles (CRIPCAS), l’Équipe SCOUP Sexualité et Couple, et le Laboratoire d’étude de la santé sexuelle. Ses travaux portent sur les déterminants psychosociaux de la santé sexuelle des individus et des couples ainsi que sur le traitement des dysfonctions sexuelles.

There has always been a stereotype that women are “more emotional” than men, and even that they are “too emotional” for leadership roles. Dr. Winny Shen joins Mind Full to discuss the results of her study which suggest that not only is that stereotype untrue, the exact opposite might actually be the case.

Jessica Strong
We all plan to get older. So why do so few of us gravitate toward working with older adults? Dr. Jessica Strong is a Geropsychologist in the department of psychology at the University of PEI. She tells us about cognitive reserve, fights against ageism, and discusses how a passion for music led her toward her current career path.
“You see the hood's been good to me, ever since I was a lowercase g. But now I’m a Big G.”
- Montell Jordan
In his monster 1995 hit ‘This Is How We Do It’, Montell Jordan makes the distinction between a “lowercase g” and a “Big G”. In his case, he’s making reference to being a young child, understanding and evincing the gangsta part before he grew to adulthood and achieved proper, professional gangsta status by releasing a staggeringly popular debut single.
Like Montell Jordan, it was music that led Dr. Jessica Strong to her eventual career path, one where she too makes a distinction between lowercase gs and Big Gs. ‘Big Gs’ are the expert specialties, Geriatrics, Gerontology, Geropsychologists like Dr. Strong. ‘Lowercase g’ refers to the little competencies everyone needs to have. Social workers, family doctors, personal support workers at retirement residences, caregivers, or retail workers. Anyone who deals with an older population in their day-to-day lives. Says Dr. Strong,
“I have a lot of students who aren’t necessarily interested in Geropsychology (big G), but we work on developing this ‘lowercase g’ workforce, which is not working with older adults exclusively. They may be a generalist psychologist, but one who has the competency to work with older adults. They understand the cohort issues and generational differences, and know how to modify an intervention or screen for mild cognitive impairment.
I tell all our clinical students ‘you want to work in paediatrics, great! How many grandparents are raising children these days? For your paediatric client, if you’re noticing something off with their grandparent, you’re going to want to figure out whether this is anxiety and stress because they’re raising a nine-year-old, or could this be a mild cognitive impairment? And how am I going to figure that out in a way that serves the interests of my paediatric patient?’”
Dr. Strong is an assistant professor in the department of psychology at UPEI, and a registered clinical psychologist who specializes in Geropsychology. Geropsychology is a subsection of gerontology – the broad study of aging, lifespan, development and identity in late life. It’s a discipline that focuses on relationships, mental health, cognition and more generally the psychology of aging.
It was music that led her toward this career path, as she started playing piano at the age of 9 and soon picked up more instruments, playing alto sax in the high school marching band. It was in high school that she started thinking about music therapy as a career. But music therapy is a pretty specialized occupation, and Jessica is someone who likes to keep as many options open as possible.
In her final year of high school, right around the time we were all learning that “southcentral does it like nobody does”, she shadowed the music therapy program at her local university. She quickly realized that there was a way to get into this while keeping more doors open, and she ended up doing two simultaneous undergraduate degrees – one in music performance, and one in psychology. The idea was that from there she could get a Master’s in music therapy if she chose that path.
But psychology research really spoke to Jessica, who started to become far more interested in the mechanisms of why music makes a difference for people, rather than just using it as a tool. She had done a little bit of work with older adults at an occupational therapy lab at Washington University in St. Louis. Then she moved to Germany, where she worked at a mental health institute for older adults, the Central Institute for Mental Health in Mannheim. She had become a lowercase g.
Soon, she realized that what she really wanted to do was work with older adults. She had never heard the term “Geropsychology” before, but she lucked into a program at the University of Louisville in Kentucky, and was accepted into their Clinical Psychology program, working under the mentorship and supervision of two Geropsychologists. She earned her Ph.D., became a Big G, and says she has never looked back.
“One of the most rewarding things about working with older adults is that they are some of the more complex human beings in the world. They’re such a heterogeneous population because they have all of the demographic differences that any of the rest of us have – gender and race and so on – but they also have all their lived experiences and the changes that have come with those. Physiological aging, emotional aging, cognitive aging. It’s really intellectually stimulating and exciting for me because they’re so much more complex than any of the other groups I’ve worked with who haven’t done as many things.”
Soon, Dr. Strong was working in Boston at a rehab facility in the Veteran’s Health Administration. She studied how integrating music into a mental health group could destigmatize talking about mental health for older male veterans. They got some great feedback, the veterans felt like this group was different from others they’d been in before, and that the use of music made it easier for them to talk about things that both as men and as veterans they’d been conditioned to avoid. Music gave them a way to feel it without necessarily having to find the words.
One of the sessions Dr. Strong did with this group used “a bit of a music therapy technique”. They would start the group session by reading the lyrics to a song aloud, like a poem. They’d talk about the imagery, and what they thought the artist was trying to convey. Then they would listen to the song to see if it felt different than just reading through it. Did the addition of music take away from the message, or did it add something? The veterans in the group, men whose gender and military service compounded a reticence to speak vulnerably, went to deep places dissecting the music.
Dr. Strong says ‘What A Wonderful World’ was a group favourite. Given the age of the participants (some Vietnam veterans, others Korean War veterans, and some survivors of World War II) it makes sense that a song from the 60s resonated as much as it did. Music is often associated with memory and nostalgia, most particularly the music we heard around major life events in our adolescence and in early adulthood. Like a wedding song, a graduation song, or one you heard while you were heading off to war.
When similar sessions are held forty years from now, there’s a good chance a psychologist like Dr. Strong will be integrating much different music into this kind of group therapy. They will discuss what Mr. Jordan is trying to convey when he suggests we “flip the track, bring the old school back”. Dementia support groups that connect people through sing-a-long music will sound like one of those Pitch Perfect mashups. “I reach for my 40 and I turn it up / designated driver take the keys to my truck”.
Music not only triggers memories, it shapes our brains as we age. Dr. Strong is specifically interested in the brains of musicians, and the effect a lifetime of playing music has on the aging process. She talks about something called Cognitive Reserve. This is the idea that everything we do in our lives builds up a reserve in our brains. Dr. Strong describes it like a battery you can charge. Having a formal education, speaking a second or third language, having strong social connections, these are factors that charge our battery and make us more resilient against cognitive impairment later in life.
“If someone has a really high cognitive reserve, a scan of their brain might look awful, with disease, or vascular damage. But they might still function okay because they’ve built up this reserve over time that allows their brain to circumnavigate those damaged pathways. Someone with a lower cognitive reserve might have a brain that looks relatively okay on a brain scan, but they might be showing signs of mild or moderate dementia in their functioning.”
According to Dr. Strong’s studies, and similar studies by her peers, musicians tend to do better in some things as they get older, like in executive functioning and language, but not in all areas. One of the areas where they don’t tend to do better than non-musicians is in memory. Some have suggested that the tests for memory are flawed, and this may be the reason we don’t see a correlation between that and musicianship. When Dr. Strong takes a sabbatical next year, this is one of the things she’s hoping to learn from a longitudinal data set she has collected. But she has learned a lot already from her research up to this point.
“I’ve compared people who retired from playing versus those who continued to play. That was an interesting study, where I found that people who stopped playing lost the benefit they had in some of the more fluid abilities like executive functioning, but maintained the benefits they got in crystallized abilities, things like language. People who continued to play continue to have both benefits.”
There are many challenges to working with older populations, in particular defining what those populations are. The general (Dr. Strong says arbitrary) line at which Geropsychologists and Gerontologists start looking at people as “older” is the age of 65. But they’re also working with people who are much older than that.
“What gets complicated about using 65 as the arbitrary cutoff is that you’re still including people who are 80, 90, even over 100. There are people over 100 participating in research, and you get into this really interesting scientific conundrum of having people who span 30 or 40 years in a scientific sample. Which is absurd – never would we put 10-year-olds and 50-year-olds in the same sample, and this is somewhat of the same construct.
So this is a problem when we work with older adults, and a lot of Gerontology and Geropsychology splits those groups up into the ‘young old’ (65-74), ‘old old’ (75-84) and ‘oldest old’ (85 and up), trying to get a little more nuanced perspective. These people grew up in completely different ways and in completely different cohorts. And a 65-year-old shouldn’t and wouldn’t be expected to be in the same life place as a 95-year-old.
It's a lot easier to get access to research participants who are in that young-old group, so they tend to be overrepresented in research. It’s a lot harder to get a representative sample for the older groups.“
Another challenge is ageism. This is something that matters a great deal to Dr. Strong, and she gets impassioned when she talks about the ways we neglect our older population. Age is a diversity factor that is often overlooked, and Geropsychologists are constantly reminding their organizations, and anyone who will listen, that age must be thought of and included as a diversity factor. Not valuing older adults, the negative attitudes we have about getting old, looking old, and acting old, create real-world harms. Dr. Strong says these are some of the reasons we have a lack of action in overhauling Canada’s long-term care system.
“We know what works in long-term care, it’s just a matter of putting it in place. It wasn’t necessarily intended to be this medical-type institutional facility. People don’t want move there because it signals the beginning of the end, and they think that because of how those facilities work. They’re understaffed, underprioritized. Some of the most amazing models of long-term and dementia care are in Scandinavia. There are enclosed ‘dementia villages’ where people live in their apartments, but they can go shopping and go wander in the park. The person cutting the grass is a trained dementia nurse, as is the barista at the coffee shop. But many of us don’t see older adults, and particularly older adults with dementia, as important enough to care.”
We’re all going to get older. As Dr. Strong tells her students, “if you’re not aging you’re dead – we are privileged to grow older”. So why are there difficulties in recruiting young people, and students in particular, to work with older populations? Ageism, like negative attitudes or death anxiety, are big factors. So is exposure. Young people who have grown up around older adults, or who have teachers or parents who work with older populations, tend to be a lot more receptive.
“I attribute a lot of my interest in aging to my great-aunt Lila. My mom was her primary caregiver when I was growing up, so she spent a lot of time at our house and I spent a lot of time with her. I found her to be fascinating. She wore a wig and I saw her without a wig which was fascinating when I was nine. She told me stories about having a pet rat when she was my age and it was amazing to think about her having ever been my age. I had good relationships with my grandmothers and I had older adults in my life a lot when I was growing up.”
Geropsychology, as a relatively new field, is an exciting one. There is an enormous breadth of research that has yet to be done, and there are countless opportunities to work with people whose life experiences, wisdom, and stories are both fascinating and instructional. They represent a living history of a time the rest of us did not experience, and have lived lives we can’t imagine. Dr. Strong says it’s impossible to overestimate how rewarding this work can be.
“This is a group that has been marginalized, that doesn’t have much of a voice, and when you take the time to interact with them they are so grateful. They have so much wisdom and so many experiences that I can’t help but learn from them. They’ve lived in times and done things that will never be available to me.
The community of Geropsychology and gerontology is such a welcoming one, because we want people to work with older adults. And because the people who end up in that field are warm and welcoming by nature. It’s just a wonderful professional home.”
We need the Big G experts to learn more about aging and about creating a welcoming, flourishing, and healthy society for people as they get older. We also need everyone else to develop lowercase g competencies, so we too can be part of the solution. As each of us gets older, we will want the world around us to change so that we can continue to build community and live meaningful, impactful lives for as long as we are around. This is how we do it.
Research papers:
Mental health and music group development and evaluation (with manual published in the appendices)
Two articles on cognition in older adult musicians
- https://www.sciencedirect.com/science/article/abs/pii/S0278262622000410
- https://journals.sagepub.com/doi/abs/10.1177/0305735618785020
And one recent on attitudes towards older adults

Laura Thomas-photo by Erik McRitchie

B.I.G. at the North Pole photo by Edel Kieran
Training astronauts for space flight requires a huge team, including psychologists who can help to prepare them for the close quarters and isolation for long periods of time. Laura Thomas is not only one of those psychologists, she has also experienced similar close quarters and isolation with all-female expeditions to places like the North Pole.
We kick off 2025’s Psychology Month: Women in Science with a look at Laura’s work, her travels, and the requirements for setting a Guinness World Record!
I am often in awe of the people I interview, many of whom are remarkably accomplished and doing work that matters to the world. At times, I’m even a little bit envious, in that I would love to have been a part of some of those projects. I confided as much in Laura Thomas toward the end of our Zoom meeting, but told her she is an exception. Not that I’m not in awe of everything she does – I certainly am. But I am not the least bit envious. I would love to have been a part of the World’s Most Northerly Cocktail Party (scroll down for canapé recipe). But very few forces on Earth could have convinced me to be part of the intrepid group that skied, camped, and braved the shifting ice of the North Pole for days in order to get there.
Laura Thomas, on the other hand, couldn’t wait. In 2016, she was a counseling psychologist in the UK and an afficionado of adventure tourism. She began to take an interest in extreme environments, and attended a lecture by British explorer Felicity Aston, MBE. They chatted, and before long Laura was joining her on a trekking trip to Ethiopia. A few years later, she was headed to the North Pole, living in Calgary, and going in a whole new direction with her career.
Trekking to the North Pole seems like a long way to go…because it is. Consider this – the distance to the current magnetic North Pole from Alert, Nunavut, the northernmost inhabited place on Earth, is a little over 800 km. The distance from the Earth to the International Space Station is only 400 km.
Do you ever look up at the ISS as it passes over us, and wonder what the astronauts are doing? Some kind of science, one assumes, and lots of freeze-dried cuisine? Some kind of exercise that looks like that scene in 2001: A Space Odyssey? As Canadians, we know that some of them practice David Bowie tunes on guitars, since there’s no way Chris Hadfield was able to do that performance without practice.
Laura knows what the astronauts are doing. Or, at least, what they could do. And how they can do it, what with the long months of isolation, the forced intimacy of close quarters, and the physical changes one undergoes while in those conditions. Laura studies people, and their behaviour, in extreme isolation.
Laura is the co-founder of PARSEC Space, a new company that exists to train commercial space operators. She works alongside scientists, pilots, and engineers from the likes of NASA, ESA, and the military to select, train, and develop the next generation of astronauts. These will not necessarily be space travelers who will be going to the ISS. There are many other plans for space exploration. Says Laura,
“Rather than space tourism, per se, we’re focused more on research and payload specialists. People who are going to go up and offer their expertise for various projects and research that’s being done in space. The thing about government agency astronauts is that it takes a huge amount of time and money to train them. And they’re generalists. They’re not necessarily the experts in the kinds of technology they’re trialing or the experiments they’re running up there. In the future there will be a lot more space research.”
Pharmaceutical companies, for example, want to test new medications in space. Things act differently in space because of the conditions. In microgravity, bacteria grows differently. There could be a lot of benefits from observing how things grow in the absence of gravity. Manufacturing companies are also leaning toward testing their products and systems in space. NASA is looking to build a permanent base on the moon, which would undoubtedly include a significant research facility.
When that happens, PARSEC will be there to train the astronauts who will go there, and Laura will be assessing the mental fitness of participants and training them to handle the rigours of space travel.
“The qualities that are desirable in an astronaut have changed a little over the years. We call it the ‘new right stuff’. Previously, missions were relatively short, so you needed people with the technical skills to get the job done. But if you’re looking at people surviving and thriving in space over the longer term, with that level of extreme isolation and confinement, you need to look at how people cope. Their innate resilience, their capacity to cope with different types of stressors, how well they get on with other people, how well they function within a team. The so-called softer side, the personality-related traits, become much more important.”
Laura can’t just go up to space to watch people and guide them in that exact environment, at least not yet, so analogue environments on Earth (those with the most similarities to conditions in space) will have to do. Subterranean cave systems, remote jungles and mountains, and of course polar regions. Laura, for example, was the crew psychological officer on one such “analogue” in the Mojave Desert where they were isolated for ten days.
“It was really interesting, we were in this habitat, which was a series of pods, basically. Eight women by ourselves, isolated in the Mojave and living like astronauts. We had a medical officer, an engineering officer, a crew commander. Our daily routine involved exercises and activities that we would need to do as astronauts.”
While there, Laura observed and assisted her crewmates to ensure everyone was coping well, identifying the best interventions and adaptations in that setting. It was the first ever analogue that was all-female, attracting scientists from all over the world. There were crew members from Jordan, New Zealand, the U.S. and elsewhere. It enabled Laura to further her research into salutogenesis in analogue environments. Salutogenesis refers to a focus on the factors that promote health, well-being, and positive outcomes for people.
A lot of people have very positive experiences in these kind of environments. Often, astronauts who go into space can look back on the Earth through the Cupola windows, which can create a profound feeling of transcendence. They come back to Earth with a different sense of the planet’s beauty and it’s fragility and develop more compassion for humanity. This is called the ‘overview effect’, and it lasts much longer than just the moment an astronaut looks out the window of a spacecraft. States of extreme awe and transcendence have also been seen in terrestrial-based analogues.
“You can see from a distance that the Earth is all landmass and water. We can’t tell where the border to one country begins and another ends. It gives you a real conviction that we’re all part of the same thing.”
There have also been reports of increases in feelings of personal strength, better stress resilience, and long-term physical health outcomes. Sometimes, the more stressful the situation is for the participants, the more profound the changes to their psyche. Laura says it’s almost like there’s a threshold of stress that must be met for the more positive benefits to take effect.
It’s hard to imagine an expedition more stressful than one to the North Pole. In 2024, Laura and her fellow explorers, all women, set out to take ice, snow and water samples at the 1996 position of the magnetic North Pole. The B.I.G. (Before It’s Gone) expedition had been planned since 2020, but delays caused by COVID and the Russian invasion of Ukraine meant that some team members had to drop out and Laura could step in.
Their team, led by British explorer Felicity Aston, MBE, trained in cross-country skiing in Norway and Iceland for weeks. Then they flew into Iqaluit, then to Resolute Bay, then to Isachsen – an abandoned weather station from the 70s which was the closest landing strip to the magnetic pole. Each of those plane flights was delayed by severe weather, which truncated the time they had to set off. On skis, pulling their equipment in their sleds, they headed toward the pole.
There were more delays along the way. Terrible weather had them stuck in their tents for almost three days. Despite being physically exhausted and seriously dehydrated, they had to push forward anyway to get ahead of an incoming storm. The team was always on lookout, for both shifting ice and polar bears. Says Laura,
“It’s an experience, but it’s hard. Being in those environments, anyone will tell you it’s hard. You need to have the right gear, but even then it’s brutal. You’re basically out there where everything’s trying to kill you. The cold, the sea ice, and even polar bears. When we got to Resolute Bay, the locals told us it was polar bear mating season and we’d definitely have an encounter with them.”
Along the way, the team collected data. They showed that all kinds of different microplastics have made their way into the North Pole ice, as have heavy metals like lead, and, importantly, black carbon. Black carbon is what is produced when we drive cars, run industrial plants, and experience wildfires. Its presence in the arctic ice is quite serious – the small black particulates make the ice melt faster than it already is, and this speeds up the effects of climate change.
Laura gathered data as well, for her salutogenesis project as she learned even more about how people respond when pushed to such extremes. Sadly, they didn’t quite make it to the magnetic north pole, thanks to the weather delays and shortened time frame for the trip. But they did stop to set a Guinness world record!
World records, at least as adjudicated by Guinness, are kind of a funny process. You have to contact them directly ahead of time, laying out your intention to break some previous world record, or create a new one (hi Guinness, it’s me! I plan to make the world’s largest Build-A-Bear, would that qualify for inclusion?) Then they have specific criteria that must be met in order for you to lay claim to that record.
And so it was that the B.I.G. team, in addition to their scientific equipment and survival gear, carried cocktail glasses, cocktail dresses, and a device to play music all the way to the North Pole with them. One of the trip’s sponsors was an alcoholic beverage company (Axia Spirit), and this was a tip-of-the-hat to them. But according to Guinness, it is not a cocktail party without tunes, a table, cocktail attire, and canapés.
An adventurous spirit, a quest for knowledge and experience, and a determined toughness made Laura Thomas an ideal candidate for a skiing trip to the North Pole. A dedication to comfort, a lack of physical fitness, and a penchant for variety in my cuisine made me the ideal person to sit at home and write about it. And it’s fun to write about a “space psychologist”. Several years ago, there might have been a handful of those on Earth. Now, as space is opening up, so are the opportunities for a vast array of experts to ensure the safety and effectiveness of this new enterprise.
Laura’s training as a psychologist and passion for research have served her well here on Earth. She is working on projects that shed light on some of the world’s most serious problems. And it is those qualities and qualifications that will serve the next generation of explorers. The ones who will head into the most unexplored regions of our world – those beyond our world. They will be in a position to succeed, thanks to a dedicated team of experts to help them with their work, and Laura to help them with their minds. Who better than someone with her kind of experience to accomplish B.I.G. things?

Maureen Plante was the recipient of a 2024 CPA Indigenous Psychology Student Award for her work at the University of Calgary studying disrupted orders of eating from an Indigenous perspective.
Maureen Plante est Iroquoise-Crie-Métisse du côté de son père, tandis que sa mère est d’origine allemande. Ayant souffert d’un trouble de l’alimentation à l’adolescence, elle a été amenée à faire une recherche de maîtrise à l’Université de Calgary, qui portait sur les troubles de l’alimentation dans une perspective autochtone. Elle a grandi en s’identifiant avant tout comme Crie, une communauté autochtone qui se souvient encore de l’époque où les bisons parcouraient les plaines canadiennes en vastes troupeaux quasi infinis.
L’éradication des bisons des plaines occidentales de l’Amérique du Nord au cours des 18e et 19e siècles est une illustration frappante du conflit entre les traditions autochtones et la philosophie coloniale européenne. À la fin des années 1700, on estimait à 30 millions le nombre de bisons vivant dans les grandes plaines nord-américaines.
Jusqu’à cette époque, les peuples autochtones de l’Ouest canadien vivaient aux côtés des bisons, qu’ils chassaient pour leurs fourrures et leur viande. La terre était un partenaire partagé qui assurait la subsistance de la population. Lorsque les colons sont arrivés, ils ont introduit une mentalité différente, celle de l’exploitation des ressources et du capitalisme. L’abondance de bisons des plaines et de bisons des bois permettait de réaliser d’énormes bénéfices sans grand effort, et la chasse a commencé sérieusement.
Pour les populations autochtones, cela signifiait qu’elles devaient elles-mêmes s’adapter à la nouvelle réalité. Elles devaient désormais entrer en concurrence avec les chasseurs blancs pour le moindre animal et étaient contraints, pour survivre, de passer d’une relation de coopération à une relation d’exploitation des ressources. Beaucoup sont devenus des chasseurs de bisons nomades, vendant des peaux et d’autres objets en échange des nécessités de l’existence. La nourriture n’était plus une partie évidente et intégrante de la vie, comme l’air et l’eau, mais une marchandise.
Il serait exagéré d’établir un lien direct entre l’éradication du bison et les troubles de l’alimentation qu’a connus Maureen Plante quelque 200 ans plus tard. Mais en même temps, il ne faut pas négliger ce lien. Ces dernières années, les traumatismes historiques ont fait couler beaucoup d’encre, notamment en ce qui concerne les souffrances subies au fil des siècles par les peuples autochtones du Canada. Mais nous commençons à peine à effleurer la surface de ce que cela signifie vraiment, et la façon dont les traumatismes historiques nourrissent les problèmes que nous observons aujourd’hui.
Maureen a grandi dans une très petite collectivité située à l’extérieur d’Edmonton, où l’accès aux services était très limité. Lorsqu’elle a développé un trouble de l’alimentation à l’adolescence, il y avait très peu de ressources dans sa région immédiate, et même dans les centres urbains voisins, il n’y avait guère de soutien centré sur les Autochtones. À l’âge de 16 ans, Maureen s’est juré d’aider d’autres personnes qui avaient le même type de comportements alimentaires perturbés, et elle n’a jamais cessé de poursuivre cet objectif depuis.
Elle a obtenu son baccalauréat avec spécialisation en psychologie à l’Université MacEwan d’Edmonton, sa maîtrise à l’Université de Calgary et elle prépare actuellement un doctorat en psychologie du counseling à l’Université de l’Alberta. Au cours de cette période, elle a travaillé au Eating Disorder Support Network of Alberta de différentes manières, notamment comme bénévole. Bien que Maureen ait toujours parlé ouvertement et avec vigueur des comportements alimentaires perturbés, ce n’est que lorsqu’elle a obtenu sa maîtrise qu’elle a pu commencer à explorer les points de vue autochtones dans le cadre de son travail.
À cette fin, Maureen a travaillé avec des femmes autochtones – thérapeutes, psychologues, travailleuses sociales – qui proposaient des thérapies fondées sur le modèle IFOT. L’Indigenous Focusing-Oriented Therapy (thérapie autochtone axée sur l’individu) est une modalité thérapeutique historiquement pertinente et adaptée, qui adopte une approche de la guérison basée sur les forces. Elle correspond à ce que font les chercheurs et les praticiens autochtones lorsqu’ils travaillent avec des Autochtones. La « grand-mère de l’IFOT », Shirley Turcotte, a travaillé avec Eugene Gendlin, créateur de la FOT, pour créer cette approche, estimant que les points de vue autochtones étaient négligés, en particulier la relation que nous entretenons avec nos ancêtres et toutes nos relations.
Maureen, qui prépare actuellement son doctorat, a déjà reçu le Prix pour les étudiants autochtones 2023 de la SCP pour le travail qu’elle accomplit et qui cherche à approfondir tout ce qu’elle a fait jusqu’à présent.
« J’ai entendu les praticiens qui dispensent l’IFOT, je veux entendre dorénavant les Autochtones. Certaines femmes vivant dans des centres urbains m’ont raconté qu’elles avaient vécu des perturbations des comportements alimentaires et qu’elles s’étaient parfois rendues à l’hôpital pour y recevoir des soins. Cela ne les avait pas aidées. Je souhaite également comprendre le rôle que jouent les traumatismes historiques dans le développement de comportements alimentaires perturbés chez les Autochtones, car j’ai l’impression que cet aspect a été négligé.
Les troupeaux de bisons n’ont jamais été près de se reconstituer complètement, et on estime aujourd’hui à 20 000 le nombre de bisons sauvages vivant en Amérique du Nord, soit 0,0007 % de ce qu’il était il y a 200 ans. Pendant ce temps, les communautés autochtones qui pratiquaient l’agriculture depuis des centaines d’années ont dû modifier leurs pratiques, car l’accent était mis désormais sur les monocultures.
Autrefois, les arêtes des poissons de la rivière fertilisaient les haricots qui fournissaient de l’azote au maïs. Les gens se nourrissaient de poissons, de haricots, de maïs et de courges qui étaient cultivées autour des cultures pour les protéger des animaux affamés. Lorsque le gouvernement canadien a commencé à construire un chemin de fer à travers le pays, la marchandisation de l’agriculture a été l’un des moyens qu’il a utilisés pour priver les populations autochtones de leurs droits. Dans cette région, on cultivait désormais de l’orge, et uniquement de l’orge. Dans cette autre région, c’était du lin, dans la région voisine, c’était du canola, tout cela dans le but d’expédier et de vendre le produit.
Les communautés autochtones agraires ont dû soit modifier leurs pratiques pour participer à ce nouveau paradigme, soit se déplacer vers des zones moins fertiles pour essayer de pratiquer une agriculture de subsistance, en espérant pouvoir cultiver suffisamment pour faire vivre leurs familles d’un hiver rigoureux à l’autre. Toutes n’ont pas pu le faire.
L’une des notions centrales de l’IFOT c’est qu’en se concentrant sur soi-même, on peut trouver son propre « remède », c’est-à-dire ce qui fonctionnera pour soi pour traiter ses problèmes de santé mentale. Lorsque Maureen a fait sa maîtrise, elle a été initiée à cette pratique. Pour elle, cela a fait remonter beaucoup d’herbe et de blé, et elle a découvert que le blé était son remède. C’était une prise de conscience étrange, car son trouble de l’alimentation faisait que son cerveau lui disait que le blé était mauvais. Cette révélation a changé son point de vue sur sa relation avec la nourriture et l’a éclairée sur le croisement entre l’identité autochtone et les comportements alimentaires perturbés.
« L’une des choses les plus importantes qui ont été partagées par les aînés et les porteurs de connaissances est la suivante : “Le DSM-5 [Manuel diagnostique et statistique des troubles mentaux, la classification standard des troubles mentaux utilisée par les professionnels de la santé mentale] est basé sur des catégories dans lesquelles on retrouve différents types de troubles du comportement alimentaire (anorexie, boulimie, etc.).” Les gardiens du savoir autochtone affirment que ce type de pensée eurocentrique rompt l’interconnexion. Ma recherche de maîtrise soulignait vraiment l’interconnexion et l’enracinement dans le contexte du colonialisme. Depuis le contact avec les Européens et tout au long de l’histoire, l’accès des peuples autochtones aux aliments traditionnels et aux droits de chasse, entre autres, a été très controversé. Beaucoup de choses se sont passées ici, qui ont modifié notre relation avec la nourriture et notre lien avec la terre. Comme la Loi sur les Indiens, des lois qui ont des répercussions sur notre relation. Un aspect sur lequel j’ai vraiment insisté dans ma recherche de maîtrise était la nécessité de commencer à changer notre relation avec le terme « troubles de l’alimentation » afin de ne pas les pathologiser, mais plutôt de les situer dans le contexte du colonialisme ».
Dans le cas des comportements alimentaires perturbés, le poids, la forme du corps et l’idéalisation de la minceur sont des préoccupations très présentes, du moins, en Amérique du Nord où le DSM-5 est le plus utilisé. Maureen est curieuse de savoir si cette idéalisation de la minceur est un phénomène qui touche toutes les cultures. Il est difficile d’obtenir des données sur les taux de comportements alimentaires perturbés chez les Autochtones et sur la répartition entre zones rurales et urbaines, car la plupart de ces données proviennent des programmes de traitement, auxquels très peu d’Autochtones sont inscrits. Certains chercheurs non autochtones affirment qu’il faut que les Autochtones s’expriment davantage sur le sujet.
« Beaucoup d’articles que j’ai trouvés parlent encore du DSM-5, du taux de prévalence, etc. La dimension narrative fait défaut, et nous ignorons un grand nombre de choses, ce qui, je le crains, nous amène par inadvertance à mettre des étiquettes sur les Autochtones (ou même sur les non-Autochtones). »
Maureen est en passe de devenir une voix autochtone forte sur le thème de la perturbation des comportements alimentaires. Son histoire se nourrit de son expérience personnelle, mais aussi de la décimation de la population de bisons, du passage à l’agriculture de subsistance, de la famine qui régnait dans les pensionnats et de toutes les autres indignités qui ont bouleversé la relation des peuples autochtones avec la terre et leur nourriture. Son avenir se nourrit de cette histoire, mais aussi de l’IFOT, du DSM-5 et d’un parcours universitaire remarquable et primé dans certains des meilleurs établissements d’enseignement supérieur de l’Alberta. Nous sommes impatients de découvrir les enseignements précieux que cet avenir radieux nous apportera!
Questions pour faire connaissance
Avez-vous un livre préféré?Je crois que oui… Les Méditations de Marc Aurèle. Il y a quelque chose dans ce livre qui fait vraiment réfléchir, qui est philosophique et qui donne de bonnes leçons de vie. Je suis quelqu’un sur les médias sociaux qui en parle beaucoup, et cela m’a donné envie de m’y plonger. Je l’ai lu entre ma maîtrise et mon doctorat, et je me concentrais vraiment sur la psychologie. J’ai trouvé que la TCC comportait un élément de questionnement socratique, et ce livre semblait intéressant à lire dans cette perspective. Lors du congrès de la SCP de 2022, j’ai assisté à une présentation donnée par deux messieurs sur le stoïcisme et la TCC, qui m’a fait penser aux Méditations et m’a donné l’impression d’une certaine convergence de vues avec les miennes!
Si vous pouviez être une experte dans un autre domaine que la psychologie, quel serait-il?
Quand j’étais plus jeune, je voulais devenir biologiste marine. J’aime les animaux, et je suis folle des raies. Récemment, j’ai beaucoup lu sur le comportement des loutres. Je sais que des recherches sont en cours sur les loutres et que les chercheurs travaillent avec les communautés autochtones pour savoir comment favoriser les relations entre humains et loutres.
J’ai lu une étude sur les loutres et les dauphins, car les loutres et les dauphins peuvent tous deux utiliser des outils, mais les loutres ont précédé les dauphins en ce qui concerne l’utilisation d’outils.
Avez-vous un sport préféré?
Non, pas vraiment, mais j’ai commencé récemment à regarder le hockey avec mon copain. J’aime aller au centre d’entraînement physique et être active, alors je fais de la musculation et d’autres choses de ce genre.
Si vous pouviez passer une journée dans la tête de quelqu’un d’autre, ce serait qui?
Je pense que c’est parce que je suis à ce stade de ma vie, mais je dirais mon conjoint. C’est un charpentier certifié Sceau rouge et son travail est complètement différent du mien. Il travaille de ses mains, c’est un as des mathématiques, et il est capable de visualiser un espace et de savoir comment y configurer les choses. C’est un travail difficile, et j’aimerais vraiment passer une journée dans son cerveau pour comprendre son univers et sa façon de voir les choses. J’admire les gens de métier, qui font des tas de choses extraordinaires, et je reconnais que je ne suis pas très douée pour tout ça! En outre, en tant qu’êtres humains, nous ne savons pas vraiment comment nous sommes reçus par les autres!
Quel est le concept psychologique qui vous a le plus surprise lorsque vous en avez entendu parler pour la première fois?
J’ai fait un baccalauréat en psychologie sociale, et j’aime encore beaucoup cette discipline. Je pense à l’étude de la prison de Stanford, l’expérience de Asch, qui font ressortir, en quelque sorte, le côté sombre de l’expérience humaine, et je trouve tout cela vraiment fascinant. Aussi, tout ce qui a trait à la personnalité me fascine, comme le modèle de personnalité à cinq facteurs. En ce moment, je lis des travaux de chercheurs qui parlent de cela dans le contexte du travail, des études, etc.
Si vous ne pouviez écouter qu’un seul musicien ou chanteur jusqu’à la fin de votre vie, ce serait qui?
J’aime beaucoup la musique classique, alors je répondrai Bach.

Trinity Stephens was the recipient of a 2024 CPA Indigenous Psychology Student Award for her unconventional work as an undergrad at UBC.
There are certain things we expect from other people in terms of their behaviour. We expect people to turn right when their right turn signal is on. We expect that when we order a coffee that the barista will put it in a cup, and that fellow bus riders will refrain from doing chin-ups on the hand-hold bars. Or, that when we get on an elevator, everyone will face the door and the buttons, avoid eye contact, and ride up to their floor in silence. And these expectations are mostly confirmed by others. Unless, perhaps, you get on an elevator with Trinity Stephens.
“Even when I was a child I never did what other people did, but it was when I became a psychology student that I realized how odd it is. We had this one social psych class where the prof sent us on missions. Like, go into society and break social norms. So for a week straight, I would go into the elevator and face everyone. While everyone faces the one direction, I was looking the other way. Just forcing myself to overcome the idea that I had to do what everyone else was doing. People hated it, especially if I was with my friends. They got really annoyed with it, and I could see the anxiety it provoked in people.”
Trinity is going into her final year of her undergrad at UBC. She’s Mi'kmaq, Métis, and Jamaican, and recently received a CPA Indigenous Psychology Student Award for her work in school – where she is doing a bachelor of arts with a psychology major, and also a minor in law & society and a minor in education.
Ever since she was a child, she had an instinct to help other people. A psychology course in high school intrigued her, and she became rapt with the idea of learning about the actions of people, and the motivations for those actions that often go unnoticed. Soon, she was looking to start an undergrad in psychology, with the goal of one day becoming a counselor for people in her community.
Trinity visited the UBC campus and immediately fell in love. Coming from the chaotic, bustling environment of Toronto, the feel of a community network, in close proximity to nature was appealing – and something far different from her familiar hometown feel. She says she feels peaceful while she’s there.
“There are actual forests on campus, and there are cherry blossoms all over, and there’s even our own Zen garden that’s really well kept up. I thought if I’m going to spend any time anywhere doing anything, I want it to be for psychology and I want it to be here.”
While at UBC, Trinity has been working at the Alpine Counseling Clinic in Vancouver as a neurofeedback technician. She works on weekends, where she sees anywhere from 4-12 clients a day, ranging in age from 4-80 years old. As Director of Feedback, she’s providing what she calls a Western form of healing, a dynamic she finds very interesting. She has 30-minute sessions with clients helping them “connect with themselves”, honing in on how they’re feeling inside and what’s causing stress and anxiety in their lives.
The connection between Western ways of healing and traditional ways is a subject of particular interest for Trinity. She is enthusiastic about both and believes that the one can enhance the other and vice versa.
“My main goal was to be a counsellor for BIPOC people, specifically in Black and Indigenous communities. There’s a lot of stigma around therapy because it’s something we’re not really used to, but it is something all our ancestors have done. So I thought that by being able to study the Western side would give me an advantage because I already have a lot of my ancestral and holistic knowledge. Even while studying psychology, I’ve noticed there’s a lot of overlap with traditional medicine and traditional ways of healing. It made it a natural thing for me to learn.”
Her love for UBC and the campus community led Trinity to apply for her Master’s program there – and only there. She was not accepted, so for the time being she is considering some other options before once again trying for her Master’s. One option might be becoming a life coach for post-grads, recognizing how much of a whirlwind it is for them right now. Another option is to become a doula.
Doulas help mothers through their pregnancies. They work with them up to the point of giving birth, and also work with them after the birth to help with things like feeding and support. Says, Trinity, “it’s especially helpful in Black and Indigenous communities to help mothers with their birthing journeys, reducing trauma for both the mother and the child. I think that would be a really nice accent to my resume when I do apply for the Master’s in the future. It can also be really expensive so I want to have a sliding scale for people who might not otherwise be able to afford it.”
It would be an unconventional choice of gap year activities, but unconventional choices are on-brand for Trinity. Iconoclastic thinking, an embrace of numerous ways of knowing and healing, and a desire to help the people around her suggest that no matter what Trinity chooses to do, her communities will be all the better for it.
Get to know me questions
- You can listen to only one musical artist/group for the rest of your life. Who is it?
- Do you have a sport? What is it and do you watch, play, follow it?
- Favourite book
- Favourite quote
- If you could spend a day in someone else’s shoes who would it be and why
Psychology Month 2024 was on the subject of climate change and psychology’s role. Our communications specialist reflects on the campaign, the key messages, and the next steps we can all take in tackling the biggest threat of our lifetimes.
Reflections on Psychology Month, climate change, and the path forward
My name is Eric Bollman, I’m the communications specialist at the Canadian Psychological Association. I am introducing myself here because I don’t normally write from my own perspective – I am usually writing about others, or their work. I thought I would write this final Psychology Month article from a personal perspective, as I have learned a lot over the course of this month and I want to share that – but I also want to make clear that these are personal opinions and perspectives from what I have gleaned. In our weekly Psychology In The News email that I send to membership, this would go under the ‘Blogs and Opinion’ section.
I started writing this piece with the explicit intent to walk the fine line that action on climate change demands – the acknowledgement that it is a crisis that can terrify many, if not most of us, but that framing it positively is the only way to encourage people to get on board in taking action. Upon re-reading what I initially wrote, I realized that despite my stated intent of looking to strike that balance, I had absolutely not done so. In fact, I had spent so much time immersed in the topic of climate change and online disinformation that I didn’t notice the negativity that had seeped into my thought process and permeated most every sentence I wrote, until I stepped away for a few days.
I feel like this is something that happens to many of us, so I hope the personal anecdotes I relate through this final Psychology Month article are helpful and, perhaps even a cautionary tale! What follows are the things I took away from the multitude of conversations I had this month. I present three areas where I think psychology can help the most, and where we can all (psychologists and non-psychologists alike) focus our efforts and attention.
Frame the conversation – and the solutions – in the most positive terms possible
It was clear to me, from the beginning, that the framing of Psychology Month in a positive way around climate change would be difficult. So much so that when I tried, I initially failed to do so. This is the most existential threat we all face right now, and in coming years it will become more chaotic and more catastrophic. It’s objectively terrifying. The more we talk about the climate crisis, and the circumstances that face us now and in the coming years, the more (rightfully) frightened we become.
That said, framing the conversation around climate change as a terrifying one is, generally speaking, not helpful. Doing so produces anxiety, fatalism, and actually discourages people from working toward solutions. Imagine being a child and learning about melting polar ice, disappearing species, sea level rise – and trying to imagine a happy future. As Paul De Luca, a student at the Prime Family Lab at York University says,
“By drawing upon the principles of positive psychology, and focusing on subjective well-being, we can potentially integrate our relationship to the environment to bolster or foster positive mental health outcomes in children and adolescents who I think are probably the most affected by anxiety because it’s their future at stake.”
Paul is right – a focus on subjective well-being can both alleviate distress and anxiety and also bolster pro-environmental behaviours. In her TED Talk, and her conversation with me on the CPA podcast Mind Full, Dr. Jiaying Zhao makes this point over and over. I believe she will make it once more at her upcoming plenary address at the CPA convention in June. There is no reason why pro-environmental behaviours can’t make us happy. Being outside on a bicycle makes people healthier, and as a result happier. Why not integrate that into our daily lives? For many people (me included) getting outside in the summer and tending to a vegetable garden can produce a great sense of peace (and a great crop of peas).
Every person in the world contributes to climate change in some way. There is no way to avoid it all. Every time I get into my car I think about it. When I make the decision between running the dishwasher and washing pots and pans by hand, I’m subconsciously calculating the impact of one versus the other. Thinking about things in this way can overwhelm us – and has overwhelmed me at times. Taking concrete steps that I know are good (maintaining my indoor garden, planning meals so I use up all the vegetables in my fridge) can take me out of a negative headspace while also boosting the health of my family.
These choices we have to make are, I think, best encapsulated by the magnificent TV show The Good Place, where Ted Danson presides over – for lack of a better word – Hell. People are making efforts to be good, and when they die they hope they’ll have been good enough to make it into Heaven – but the complexities of modern life have made it literally impossible for anyone to achieve the proper level of “goodness” and nobody new has been admitted to Heaven for centuries. Danson’s character sums it up –
“Just buying a tomato at a grocery store means that you are unwittingly supporting toxic pesticides, exploiting labour, contributing to global warming. Humans think they’re making one choice, but they’re actually making dozens of choices they don’t even know they’re making.”
There is good news in the struggle against climate change. A decade ago, part of the debate was framed as either you embrace renewable energy but sacrifice the economy and GDP, or you ignore renewables in order to ensure economic growth. Today, those concepts have been decoupled – and renewable energy is an economic driver of its own. Heat pumps, solar panels, and electric vehicles are becoming cheaper and more accessible. Major countries, and companies, have pledged to crack down hard on methane emissions, one of the most effective ways to limit global warming in the coming years. There is reason for optimism!
Holding ourselves to an arbitrary standard makes little sense. We can’t deny ourselves every pleasure for fear of our carbon footprint or impact, or we will become like Michael McKean’s Doug Forcett on The Good Place – living life in a perpetual state of anxiety where our entire world crumbles whenever we accidentally step on a snail. Instead, we can focus on making ourselves happier – and the world better – through actions that we know can do both.
Win the war on trust
As McMaster environmental science Ph.D. student Kyra Simone points out, there has long been a narrative pushed by those who would deny climate change exists – namely, attacking the messenger rather than the message. Calling out hypocrisy from those who are the most vocal about solutions as though that somehow means that what they’re saying on climate must be false. Al Gore flew to a conference! David Suzuki has houses! Greta Thunberg owns clothes! Sure – some of those things can be framed as hypocritical, but none of them makes the message a false one.
This particular kind of disinformation seems relatively recent when it comes to things like vaccination. But it has a long history in the realm of climate change, starting with oil and gas companies funding fraudulent studies decades ago to muddy the waters around the conversation such that no one could tell what was true and what was invented. Presenting those counter-narratives in a ‘scientific’ sort of way is a big reason many people continue to be skeptical of science today – particularly climate science.
We hear a lot about a War On Truth. That the current political climate and online discourse is designed to make Truth subjective – well, that may be true to you, but I have an alternative set of facts. I think really this is a War On Trust. Concerted efforts to delegitimize academic institutions, the media, and experts of all kinds have allowed charlatans and disingenuous public figures to replace the trust people once had in those institutions with trust in them, and in their podcasts and Substacks and supplement brands. These efforts have worked to some degree. Americans now trust what they read on social media more than traditional media. In Canada we’re not there yet. But we’re trending in that direction.
As someone who spends a lot of time on social media – I’m the person who puts out the CPA’s social media content and monitors the trends and responses and direct messages, I probably spend more time on social media than the average person, and (I assume) more than a psychologist would suggest is healthy. Spending time in that space, Twitter especially, is a constant barrage of people and bots who want nothing more than to contradict an expert in the area of their expertise, attack their character, and seek online clout through the most negative means possible. It becomes hard to remember that those people are a very small minority, since those platforms have made that minority the loudest one in our collective history.
I feel like Dr. Katherine Arbuthnott would tell me I’m not seeing this stuff as often as I feel like I do. Which is probably true – I can think of only twenty or so direct examples, but those do occupy an outsized place in my memory bank. She’s evangelical about the fact that we, North American human beings, have been conditioned to trust others too little. That we consistently underestimate the willingness of strangers and even friends to be helpful, to do the right thing, and to put the needs of our collective neighbourhoods and communities above some of our own.
I failed to keep this in mind throughout all of February. It was only when I was about to write an angry response to a bizarrely un-factual and conspiratorial tweet from a well-known Canadian public figure about climate change that I had to stop and take stock of my headspace. I realized I was outside the bounds I had set for myself. So what to do?
We can work on our own media literacy – does this story come from a reputable source? Are we sure the scientist who created the study being referenced is in fact a scientist? And an expert in the field in which the study was conducted? Is the story being hosted on a platform that actually fact-checks?
Another option is to counter the un-factual with the factual. I don’t mean commenting on the meme your Facebook friend shared about Al Gore being rich ergo climate change is not real. As Rachel Salt of Science Up First says, commenting or quote-tweeting or sharing a post so as to debunk it really does little more than amplify the wrong information. She suggests screenshots of the content that can then be addressed without adding to the destructive algorithms that got us here in the first place. Or, just post your own thoughts and your own science and your own content – the more truth there is online, the less able it is to be drowned out by the outsized volume of the clamorous minority.
We can trust that most of the people we know, and most of the people we meet, have a similar level of concern about major issues like climate change. We can believe that any action we take will also be taken by a multitude of others, and that doing this enough times will create the large-scale changes those actions are intended to create. And we can ignore the loudest voices in the room and on the internet, secure in the knowledge that the majority of people feel the way we do, act the way we do, and are moving toward the same goals we are.
They’re just not as loud about it – you might get internet clout for a few days by sharing a theory that Kate Middleton is in fact a Manchurian Candidate-style brainwashed operative installed in the British Royal Family in order to make cheese illegal. You’re less likely to get clout for telling people about your radish garden. And so I, a regular user of the internet, am far more likely to hear about the illegal cheese than I am about your radishes. More’s the pity.
Lean on others
The solutions to climate change are interdisciplinary. That’s a word that usually refers to experts from different spheres working together to advance a science they would not be able to do as effectively on their own. Like that time Amy and Sheldon shared a Nobel Prize on The Big Bang Theory. This is true in terms of the climate crisis as well – one scientific breakthrough builds on another, and one discipline enhances the others merely by virtue of their collaboration.
Witness the young scientists in Dr. Heather Prime’s Prime Family Lab at York University, Paul De Luca and Alex Markwell, integrating climate change into their studies with families and children. They don’t have to do the work of determining whether climate change is a threat, or is real – they can treat that as a fact and take a further scientific step from there. Environmental scientists have done that work over the course of decades, through cuts in funding, official muzzling, and the vocal skepticism referenced earlier that seeks to undo their work.
As Paul and Alex build on climate science, McMaster PhD student and Science Up First contributor Kyra Simone is creating new climate science based on decades of environmental work, and setting the stage for breakthroughs in dozens of fields for decades to come. Psychologists are combining their specialties at University of British Columbia, where Canada Research Chair in Behavioural Sustainability Dr. Jiaying Zhao has partnered with happiness researcher Dr. Elizabeth Dunn to find ways to encourage behaviours that will both help the environment and increase happiness.
In community action, emergency room doctor Dr. Kyle Merritt has partnered with many other healthcare professionals to form Doctors and Nurses for Planetary Health in Nelson, B.C. Psychologist Dr. Todd Kettner is also a member, and they learn together about ways they can make their own jobs and practices more climate-friendly (anaesthetic gases are a major contributor to global warming!) As a group, they consult with city officials on ways to improve sustainability through infrastructure projects and municipal policies.
The Environmental Psychology Section of the CPA is a section that does not specifically look at environmental issues, per se – as in pollution and emissions and disappearing sea ice – they look at peoples’ behaviour in relation to their environments. That includes physical built environments like their homes, offices, or the streets and blocks they go through on their commute. It also includes natural spaces like parks, forests, or waterways. This year they decided to create a working group to bring together psychologists of all types to work together on climate solutions. Dr. Phoenix Gillis took the first step , Section Chair Dr. Lindsay McCunn quickly got on board, and the meetings have been lively, informative, and well-attended.
Their initiative could produce some great results, with the variety of expertise psychologists bring to the table. Industrial/Organizational psychologists, who study human behaviour in the workplace, collaborate with Environmental psychologists to design climate-friendly offices where people are happier to come to work. Clinical psychologists whose patients are expressing anxiety about this existential threat can work with Social and Personality psychologists to come up with concrete actions that can increase sustainability while lessening the dread people feel.
I am the person responsible for the Psychology Month initiative at the CPA. Which meant that this year I sat with the impacts of climate disasters, the missed targets of the past several decades, and the existential dread – mostly alone. I needed someone else to point out my increasing negativity, to which I had been largely oblivious. In this case it was my wife Jen who made an offhand comment about it which elicited in me a moment of clarity. I have spoken with so many wonderful people, dozens of them, over the past four months in preparation for this campaign, but by the end I missed or forgot several of the lessons that I myself was trying to impart this month.
We can all reach out to someone we know to get on board with their work, to get them on board with ours, or to get the ball rolling on something new. We can trust that the people to whom we reach out will more often than not be of a like mind on climate change, and will embrace the chance to act. Collaboration makes us happier, and the steps we take in tandem lessen our trepidation and anxiety when it comes to existential threats.
Postscript: the Earth is a collaborator too
After finishing this article, I had one more conversation this month that I think might add a fourth area for consideration. I spoke with Kohkom Beverly Keeshig-Soonias, an Anishinaabekwe psychologist and member of the Chippewas of Nawash First Nation. We were speaking about land acknowledgements – the reason we do them and the meaning behind them.
Indigenous people have been doing land acknowledgements for thousands of years. It is only recently, in the spirit of Truth and Reconciliation, that they have invited the rest of us to join them in doing so. A land acknowledgement is much more than simply pointing out that Ottawa is the ancestral home of the Haudenosaunee, and that settlers and colonialism displaced them forcefully decades or centuries ago.
A land acknowledgement is a verbal, or written, expression of the understanding that not only did the Indigenous people live on this land before Europeans arrived, they had a relationship with that land. It’s an acknowledgement that, even though that land might now have a golf course or a Jean Coutu or the CN Tower on it, the relationship between the people and the land remains ongoing.
Kohkom Beverly speaks about land as a partner, the other half of a relationship that feeds both of you. The land provides you with food, water, and shelter. The air you breathe and the sustenance you require to stay alive. In return, you provide the Earth with what she needs. You maintain the soil, you help get water to the plants and plants to the animals and you treat her, the land, as an equal partner in a relationship that benefits you both.
It is only when we start to see the land as a thing, as inanimate, that we are able to use it, to extract resources for our own gain at the Earth’s detriment. The Indigenous people who were caretakers of the land for thousands of years, and are still caretakers of the land, would never act this way. To do so would be to abuse a partner, to ignore a relationship, to exploit a family member.
And so perhaps the final way we can approach the issue of climate change is to look at the Earth, and the environment, and the very land on which we stand, in a different way. Not as a thing we’re trying to help, or as a victim to whom we’re trying to atone for the harm we’ve done. But instead as a collaborator and an entity with whom we have a relationship. A partner with whom we are working to improve the circumstances for us both.
We have a long way to go, but we always go further together.
Throughout Psychology Month in February, the topic of disinformation when it comes to climate change has arisen time and again. To close out the month, we spoke with Kyra Simone and Rachel Salt at Science Up First about our responses to disinformation, ways to combat it, and difficult conversations with friends and family.

This summer wildfires ravaged the Northwest Territories, forcing the evacuation of about 70% of the population. Yellowknife psychologist Merril Dean was one of the evacuees, and saw the devastation from many perspectives. In this Psychology Month episode of the CPA podcast Mind Full, Merril shares her own experiences, as well as some thoughts on the government response and where the northern communities might go from here.
Starting a little more than a decade ago, climate science in Canada suffered a significant setback when the federal government cut funding for environmental research and restricted scientists from speaking with the media and sharing their findings. Climate scientists are still feeling the effects of those policies, and have still not completely regained their footing. In the interim, other scientific disciplines started taking a greater interest in climate change and making some strides. One of those disciplines was psychology.
Psychological scientists incorporate climate into their studies
When a researcher or student applies for money to conduct research, they have to convince the funders not only that their idea is a good one, but that they are the person who should be doing that research. Funders look at a lot of things including the impact of the research, the way the knowledge will be shared, the time it will take to complete, and the return on their investment (value for money).
In the Prime Family Lab at York University, lab director Dr. Heather Prime is discussing the future with her student Alex Markwell. Because of how they apply for and receive their funding, their research projects must be closely tied to the lab itself – in their case, that is the study of family dynamics. How parents and siblings influence children from birth to adolescence, or how major or minor external events affect families. The lab launched in 2020, just as the COVID-19 pandemic became a major external event that upended family dynamics across Canada and around the world.
Students come to a lab because of the expertise that the research program and supervisor bring to that lab. This is what drew Alex to the Prime Family Lab. Her area of interest is child development within a family systems framework and this is the lens through which she looks at potential projects. She has a keen interest in acting on climate change, but this was not something that was part of the discussion before her arrival. Only through conversations with her new lab director did they discover that this was a shared passion. Heather says,
“Alex brought up a year or two ago that the way we study the pandemic is really transferrable to the way we might study climate change.”
So they started thinking about ways they could integrate climate change into their established research program. As Alex thinks ahead to her Ph.D., which she will be starting in September, she has written a proposal for a scholarship focused on the pathways linking climate change to child and family well-being. One aspect of this proposal is the creation of a theoretical model from a family system perspective.
“Because climate change is going to be more and more relevant to more and more people, you need a map – which sounds annoying because it’s theoretical, but it can create a framework of ‘here’s what we think is going to happen based on everything we already know’. That takes a lot of work – you’re scouring the literature, bringing together a number of theories, and then creating this ‘map’.”
Specifically, Alex is talking about looking at how climate changes and climate change-related events may affect children’s mental health through disruptions to family functioning. She’s thinking that would be similar to the COVID family-disruption model that Heather published, about how the pandemic’s social and economic disruptions trickle down into families and affect their dynamics.
They can start looking at feasible interventions – something psychoeducational that could teach parents and caregivers how to talk to their children about climate change. Or maybe the social and economic ripple effects of climate change impacting family relationships where children may suffer, given that kids are so dependent on their relationship with their parents. First though, they must define the parameters of their study.
Are we talking about families who have experienced a major climate event – like losing a home to a wildfire – or families who are under threat of such an event (live in proximity to a flood zone) – or are we talking to families who are just generally anxious about the whole thing? Can they survey those people in Toronto?
There are many questions to answer before applying for research funding. Many more questions arise after that funding is secured.
Canadian climate scientists are still feeling stifled
Many of us remember the protests staged by scientists in 2013 over what they described as the ‘war on science’ being waged by the federal government at that time. Science funding was drastically cut, and the scientists who were still able to do research were prevented from communicating the results of that research to the public – which is kind of the point of doing research in the first place. An enormous amount of that muzzling was done around climate science, as the federal government sought to downplay the most dangerous effects – and even the very existence – of climate change.
Dr. Alana Westwood at the School for Resource and Environmental Studies at Dalhousie University researches natural resource management and science. Her lab recently completed two studies into interference with environmental research in Canada. Of the 741 environmental scientists surveyed, 92% reported experiencing interference with either the conducting or the communicating of their research. Dr. Westwood, along with her research associate Manjulika E. Robertson and Master’s student Samantha M. Chu, wrote an article in The Conversation discussing their findings and the ramifications of these pervasive invisible barriers.
Since that time, the policies at the federal level have changed. In theory, this means that scientists can get back to their work and can share their results with impunity. Alana’s studies suggest that this is, sadly, not the case.
An atmosphere of uncertainty is partly to blame – for a long time, certain kinds of science went unfunded and specifically shunned. Can scientists go back to those subjects, studying pollution and endangered species and emissions? Will they get funding if they do? What about funders – there is now a fair amount of external pressure on them to fund only certain kinds of research, pressure which has not necessarily abated just because of a change in federal policy. Alana says,
“We identified interference in two categories. One is externally imposed – when a researchers’ employer is putting restrictions on their ability to conduct or communicate their research. That could come from workplace policies, it could come from their manager, senior leadership, or their communications departments. The category we found that was new and more insidious was internalized interference. This happens when researchers themselves don’t want to communicate with the media, either out of fear of being misrepresented or of public backlash.”
Climate scientists exist within a system where the trickle-down effects of the war on science are still being felt. What has resulted is that a Canadian climate science environment that became fractured a decade ago remains fractured to this day, and important work in this space has been delayed or shelved entirely.
Back in the Prime Family Lab at York, Dr. Prime says she has not felt any external pressure that could be considered muzzling, and has not experienced any interference when it comes to the subjects she chooses to tackle. This may partly be a result of her lab being so new. It might also be because until now, her lab has chosen to focus mainly on COVID. But it’s likely that a lot of the reason is that the Prime Family Lab is a psychology lab – a discipline that has not been targeted by the same kind of scrutiny and interference over the past two decades.
Psychology has a role in the climate science conversation
“I think at this point, psychology probably has a primary role in the response to the climate crisis. Climate scientists and ecologists and environmental engineers have pretty much figured out the solutions to our problems. There’s a lot of work to do still, obviously, but now it’s more about people taking up those solutions.”
Dr. Katherine Arbuthnott is Professor Emeritus from Campion College at the University of Regina. She has spent the past couple of decades studying the health benefits of connection with - and spending time in - nature. Spending time outdoors, interacting with trees and wildlife and sun, has benefits for both our physical and mental health – and it has the added bonus of nudging us in the direction of environmental sustainability.
Katherine is quick to point out that psychology has long been a science focused on individual behaviours. What makes A person do A thing. In her time as a cognitive neuroscientist she would study individual brains to look at the processes of cognition. Clinical psychologists generally work with one person at a time, to help that individual in a personalized way that works best for them. A lot of the psychology around climate change interventions has been focused in this area.
Dr. Jiaying Zhao is the Canada Research Chair in Behavioural Sustainability and an associate professor in the Department of Psychology and the Institute for Resources, Environment and Sustainability at UBC. She has led studies like the one demonstrating that putting images of turtles and dolphins trapped in plastic debris on recycling bins and garbage cans reduced the amount of plastic waste people threw away.
“We found that when we placed those images on garbage stations, the amount of plastic waste was reduced – that is, the amount of plastic waste going into all streams, garbage and recycling alike. People are responsive to those images, and the principle is trying to connect our actions (throwing stuff away) to the downstream consequences of those actions (dolphins in distress).”
Jiaying has also launched an effort to connect sustainable behaviours with happiness. Jiaying, a behavioural scientist, collaborated with her colleague Dr. Elizabeth Dunn, a UBC psychology researcher specializing in the study of human happiness. What resulted was an idea for reframing the discussion around climate change from one of sacrifice (give up meat, shop less) to one of happiness. So many things that are better for the environment (eating more vegetables, riding a bicycle) are also things that improve our mental health and make us happier people!
Jiaying gave a TED Talk on that very subject which includes what the kids would call “hacks” to make you happier while benefiting the environment at the same time – like feng shui-ing your fridge. Or making the effort to carpool with people who can make the dreary drive in to work in rush hour traffic a more enjoyable and brain-stimulating experience.
To truly make a difference in the battle against climate change, it will take many people doing many little things, and many countries doing many big things. Individuals who do the little things are more likely to demand the big things of their communities and countries. And we’re getting there. More people than we realize are willing to take the actions that are required to stave off the worst of what climate change might bring.
Katherine speaks a lot about trust. The trust we have in other people to do the right thing, and the gap between our perceptions and the reality when it comes to the intentions of others. We, as people, tend to greatly underestimate the level of commitment in strangers to do the right thing, when in fact each of us is more likely than not to want to take actions that benefit all of us collectively. She also recognizes that truly addressing the climate crisis goes beyond simply engaging individuals to act differently.
Psychology can help. Yes, psychological science is a little late to the game. But it is now a player in the climate discussion – and can be an essential one, bridging the gap between the conclusions and solutions proposed by climate scientists and the implementation of those solutions by people and communities. Environmental scientists in Canada have been set back, and are only now starting to regain their footing. But they’ve done a tremendous amount of work over decades telling us all what’s happening and what we need to do. They are not ringing the alarm bell alone. Jiaying, Katherine, Heather, and soon Alex and many others like her will be adding their expertise in a truly interdisciplinary collaborative effort to put us all on the right path – toward sustainability, planetary health, and our own collective happiness.

So much of the talk when it comes to the climate crisis is doom and gloom. It’s hard for many not to become a little defeatist or to throw their hands up and ignore the problem. The solution to that kind of despair is action – little actions that move us all toward a more sustainable future. And those actions – and the conversation about them – can be a happy one! Our podcast guest is Dr. Jiaying Zhao, who connects climate action to our own personal happiness in a way that we hope spurs some of that action – and makes you happy along the way!
Dr. Heather Prime, Paul De Luca, Alex Markwell
A lot of action on climate change is aspirational. Pledges, pacts, and agreements are often non-binding and have no enforcement mechanisms. But aspirational action is action, and it often works – especially when the action is undertaken by many. York University’s Psychology Department is the first in Canada to sign on to the 1 in 5 Project, an initiative that asks academics and students to make climate change the subject of one in five projects or assignments.
The United Nations first recognised climate change as a major, urgent, global issue in 1992. In that year, the Rio Earth Summit resulted in the first international agreements on climate change. Then in 1997, the Kyoto protocol required developed countries to reduce emissions by 5% below 1990 levels – but developing countries (including China and India at the time) were exempt. Since that time, the developed countries have managed to reduce emissions by 17% (collectively). Germany had reduced their emissions 30% by 2020. The US backed out of the Kyoto accord in 2001.
More conferences, meetings, and summits have followed. 2009 in Copenhagen, 2010 in Cancun, 2011 in Durban, 2012 in Doha, 2013 in Warsaw. Agreements are reached, targets are set, countries back out, targets are missed, agreements fizzle.
In 2015, a landmark in climate change action was achieved in Paris. 196 countries signed on to the Paris Agreement, the most significant global climate agreement ever. The results? To be determined…countries can choose their own targets and there are no enforcement mechanisms to ensure they meet them. Since that time, there have been a lot more meetings…with mixed results.
All this said, many countries – including some of the most important ones – have made a concerted effort to meet the targets set by these series of agreements and accords and pacts. Although there is no enforcement mechanism by which they can be held accountable, the mere action of signing on to a global accord has, in fact, encouraged many of the world’s powers to move toward renewable energy and a greener infrastructure, though not nearly as quickly as many of us would like.
Climate progress is slow. But it is progress nonetheless. It may be frustrating. It may feel like it happens at a snail’s pace and not nearly fast enough considering the urgency of the issue. But it is happening, and hopefully the worst of what climate change could portend might be averted as a result.
In the past year, York University’s Psychology Department has joined the global 1 in 5 project. The project is a framework to allow the academic community to focus some of its collective brainpower on climate and biodiversity, and York is the first psychology department in Canada to sign on. The idea is that academic institutions commit to ensuring that one out of every five assignments, projects, or courses has an element related to climate change attached to it. Like other climate accords, agreements, and pacts, there is no enforcement mechanism, and no accountability – just the desire to improve the future for everyone on Earth.
Dr. Heather Prime, director of the Prime Family Lab at York University, has become a strong supporter of this project, which has meant incorporating climate change issues into her own curriculum as well as thinking about the climate crisis more regularly. The universities and institutions that sign on to the 1 in 5 project are not specifically held accountable for following the mandate. But there is still an effect. It may be slow – slower than we would like – but that is not on today’s researchers. The slow pace of social science around climate change is the result of years (and years) of avoiding the issue by the community at large. Says Dr. Prime,
“[The 1 in 5 project] serves as a kind of challenge to everyone to think about how you can consider climate change in your discipline. Moreover, it involves students in the process. In many ways later generations are more committed to the cause, because they’re the ones that will be most impacted.”
It has not been a straightforward process for Dr. Prime to implement the 1 in 5 mandate to her courses, and it may not yet be fully integrated. Her lab is specifically interested in family dynamics – how children develop emotionally within their families, how stressors on parents and caregivers trickle down to the kids under their care - that sort of thing. At first glance, this might not seem like the kind of place where researching climate change can have a major role. But it does.
As Heather, and her students, say – climate change is a factor in virtually every facet of our lives, which means it can have an impact in virtually every research project one can imagine. Not just in environmental science, but in the social sciences as well. Researching income inequality? That will be exacerbated by climate change. Depression and anxiety? For many those are made worse thanks to thinking about the impending catastrophe that faces us all.
And so, while the York University Psychology Department signs on to the 1 in 5 project, they are in the early stages of implementing it and have not yet reached the goal where 1 in 5 of their assignments is about climate change. As with so many climate change initiatives, it’s more of an aspiration than a firm commitment. But it has an undeniable effect.
Paul De Luca is a Master’s student in Dr. Prime’s Family Lab at York.
“I think the mandate of the 1 in 5 project is very motivating, because dealing with climate change can feel like a major uphill battle. But when you go on the 1 in 5 website and you see all these amazing projects that are currently ongoing, you feel like you’re part of a collective movement. And that in some ways informs the work I do, because I’m able to scroll through and see what other schools are working on and what other labs are doing. I can take that and let it inform the work I’m doing, and maybe identify some of the gaps. I think of it as a collective movement toward this shared goal of talking about climate change.”
It is sort of a soft target. One in five projects will be about climate change…eventually. But the mere act of signing on to the project, and to the pledge, has brought York’s psychology department into the conversation, and its students into the realm of climate-related science, and has encouraged them to think about their own particular specialties through that lens. Paul continues, talking about a study he saw on the 1 in 5 website.
“There was one proposed project about how childrens’ understanding of climate change and attitudes toward the environment change as a function of age. There was a fair amount of research from the adolescent perspective, but not so much from the vantage point of younger school-age children. When I see something like that, I start thinking about the measures we currently have that have been shown to work with pediatric populations. Do we have the tools to deal with things like knowledge of the climate crisis, attitudes toward the environment, and anxiety arising from that knowledge. And I don’t know that we currently do.”
Alex Markwell, another student in the lab, is working toward her Ph.D. and considering dissertation topics. She hasn’t paid much attention to the 1 in 5 project, and hasn’t looked deeply into it – her commitment to addressing climate change was a pre-existing condition. She does find the website and the fact that York has signed on to be encouraging.
“It’s nice to know there are a lot of other students who are interested and passionate in the same kind of things. I’ve mostly been focused on looking at the research that has been published over the past decade, but this is a good resource to look closer at what’s currently going on.”
For now, that is what the 1 in 5 project is for students and faculty at York – a resource. It’s also an aspiration. Changes to the curriculum so far have been minor. For example, Dr. Prime teaches an undergraduate class called Atypical Development, which is about the assessment and treatment of child mental health issues. For the past three years, she has assigned them a class activity centred around designing studies on COVID and families. This year, the assignment was focused on climate change.
The students came up with really interesting study designs. One proposed looking at how food scarcity relates to brain development. Another thought to track calls to crisis lines as a function of catastrophic weather-related events. A third proposed a study would look at recurring droughts in rural Canada and how that related to mental health issues. The students embraced the project, and for those who were feeling anxious about the climate crisis it was a useful way to channel efforts toward it. It’s a way of connecting people to their role in the outcome of the world.
The changes are small – but they are changes. The idea of the 1 in 5 project is fairly simple, that academics from all disciplines can come together to collectively tackle the biggest issue in the world, all by doing something small. This, it seems, is the path forward and the way out of the worst of the climate crisis – we don’t all have to change our lives to devote ourselves to this cause. We can all do little things, and observe those around us doing little things as well, and collectively that is a big deal for today and for the future.

Dr. Alana Westwood and her lab at Dalhousie University recently completed a study of environmental researchers in Canada. Their results showed that researchers in this space still feel muzzled despite changes in federal policy designed to allow them more freedom to speak and share their results. On the CPA podcast Mind Full we discuss the reasons for this, the ramifications, and specifically what this means for environmental science – and the communication of that science – in Canada.
Merril Dean
In the summer of 2023, wildfires forced the evacuation of 70% of the residents of the Northwest Territories. There was a lot of trauma that resulted from leaving their homes behind. But there was also the stress of figuring out how to get supports through cultural and language barriers, and the shock that came when they returned to devastated communities. Yellowknife psychologist Merril Dean provides an inside look at the experiences of the people in the Northwest Territories, and makes some suggestions as to how schools can best help their staff and students upon their return from devastating climate events like these.
The unprecedented numbers of wildfires in the Northwest Territories (NWT) in the spring and summer of 2023 saw more than two-thirds (roughly 70%) of the territory’s residents displaced from their homes. Much of the population was evacuated from their homes for periods exceeding a month. Some communities faced multiple evacuations. On May 14 at 4:30 pm, Katlodeche Reserve, was evacuated across the river to Hay River. At 11 pm that very evening, the town of Hay River had an evacuation notice issued with citizens from (now both) communities urged to go to Yellowknife or head south into Alberta. On June 6th the population were allowed to return. Then on August 12th, the population of Fort Smith was evacuated to Hay River. Less than 30 hours later the communities of Hay River and Katlodeche faced yet another evacuation, this time to Alberta, finally able to return after September 13th. Communities north of Hay River faced evacuations through August, with Yellowknife being evacuated on August 13th. In total approximately 25,900 people were evacuated from their homes in the NWT during the summer of 2023.
Gerald Antoine, Grand National Chief of the Dene Nation, has called for an independent public inquiry to encourage everyone to talk about their experiences as the NWT government’s planned wildfire review does not include public engagement.
The massive evacuations of both large and small communities in the NWT this summer highlighted problems that may not be totally unique to the north, but became much more acute because of the relative isolation and the language and cultural component of many of the Indigenous communities in the north. In the past, communities that faced evacuation were typically encouraged to seek shelter in the closest larger community within the territory, thus ensuring at least some cultural and language supports were available; however, the breadth of evacuations in 2023 sent families south. For families with their own transportation and experience with travel, the evacuations, though stressful and frightening, were manageable. For families from smaller communities, or even Yellowknife, who had limited means and no transportation, the evacuation presented bigger hurdles. Families were loaded onto planes to be flown south. They were allowed to bring only 1 small backpack per person. In a number of situations the people did not even know where they were going when their planes took off. At least one flight was rerouted in mid-air and the passengers were taken to Calgary instead of Edmonton. In some cases Elders, who are unilingual speakers of their Indigenous languages, were evacuated to cities where there were no language supports. One educator reported that her grandmother was sent to Vancouver on the medical evacuation and it took the family 4 days to locate her and have a family member travel to join her to act as a translator.
The National Association of School Psychologists wrote a 2017 article about helping children and families after wildfires. Their article talks about how massive evacuations upset security and normalcy. The need to relocate, even temporarily, causes trauma, emotional reactions and coping issues.
For children and families who evacuated the NWT by road in the summer of 2023, additional stress was created by having to drive through fire on either side of the road, while also experiencing extremely poor air quality and visibility because of smoke. During this summer, families driving out of the north drove through the community of Enterprise, where 90% of the community had been burned down a few days before the northern evacuation. The sight of the burned-out community was devasting to children and adults alike.
For some students in the NWT, evacuations caused them to experience interrupted schooling through May-June and again in September before they were allowed to go home. Those students who drove back to their communities were witness to vast expanses of burned land, and active fires still burning or smoldering. Air quality was still poor. These sights made it apparent to the children that, despite being allowed to return home, the fires were still very real and close by.
The evacuations in the north were costly for families. While accommodations were provided through the Red Cross, or local disaster organizations in communities that accepted evacuees (these accommodations were paid for by the Government of the Northwest Territories - GNWT), those who were most economically vulnerable still experienced considerable economic stress. Hourly wage earners were suddenly without income, families on income support had already spent much of their monthly stipend on food that they could not bring with them during the evacuation. Promises of funding were implied by the government, but it wasn’t until near the end of the evacuation when details were shared – and evacuation financial supports were quite minimal. As a result, children and families faced food insecurity both during and after the evacuation.
Returning to the north following the evacuation exposed families to the sight of considerable changes around their homes and communities. Houses outside of their neighbourhoods had been destroyed by fire, and the burn areas approached the communities - in some cases encroaching right into them. Driving in their hometowns, children and families were constantly exposed to reminders of the evacuation and ongoing threat. Wildfires moved underground in the north, into the peat and as a result, at the time of writing (January 2024), fires are still smoldering – issuing smoke, and sometimes bursting into flames in the burn areas. While driving the highway between communities, where there was significant burn, people are still smelling and seeing active fires. While the burns are not currently threatening homes, their very presence causes unease and worry.
The massive number of people evacuated means that everyone in every community was affected. Teachers and counsellors were touched by the evacuation and threat of wildfires, and experienced the after-effects, just as their students and their families did. The added stress of financial strain caused by the evacuations has added to food insecurity and increased financial worries for families in the north.
Steps to support staff in schools, to ensure that they can also support their students, is important. The National Association of School Psychologists (NASP) recommends that school staff be given the opportunity to share their experiences and feelings and process them so they can support their students. Staff need to be aware of possible trauma responses from their students and be prepared to share that information with parents, who might be expressing the view that their child’s behaviour has changed since the evacuations.
(Anecdotally, psychologists working in fire-affected communities are reporting an uptick in parental referrals for children experiencing anxiety and behavioural symptoms that emerged during the evacuation and have not resolved.)
Schools with counselling support should be encouraged to create group crisis intervention discussions with their students to encourage them to share their experiences, process concerns, and help them understand wildfires. In schools and districts that have school psychologists, they could be the ones leading these discussions. In the NWT there are no school- or school district-employed psychologists, but similar support could be found through mental health youth counsellors.
As the community begins to return, it is important that schools continue to provide supports that allow students the opportunity to explore and process their experiences. It’s also important to discuss concrete steps that students can take and how to involve themselves in actions that can help them develop problem-solving skills for the future.
As climate-related events cause more upheaval and disruption to large numbers of population groups, it is important that schools and systems develop plans to support both their students and their staff. As the lived experience in the NWT shows, there are stages of response – from the immediate needs that come with an evacuation to the longer-term worries, concerns and impacts that an extended evacuation will cause. School districts are encouraged to ensure they have “return to school” plans that include longer-term mental health supports for students and families. They are also encouraged to promote long-term actions regarding the climate-related crises that are becoming more and more common throughout the country.
This article by Merril Dean originally appeared in the Fall-Winter newsletter of the CPA’s Education and School Psychology Section.

We kick off Psychology Month in February speaking with Dr. Katherine Arbuthnott about trust on the CPA podcast Mind Full. We tend to think of other people as self-interested, and we are therefore pessimistic about things like our ability to tackle major subjects like climate change. Dr. Arbuthnott is here to tell us this isn’t really the case – that most people are, in fact, willing to make sacrifices for the good of the communities and the people around them.
Dr. Todd Kettner and Dr. Kyle Merritt
Nelson, BC was right near some of the most extreme and devastating climate events of 2021. The heat dome and wildfires had a profound effect on the city and the surrounding area. Dr. Todd Kettner and Dr. Kyle Merritt stepped up to do something about it in their own practices and workplaces. Dr. Kettner is a practising psychologist and Dr. Merritt is an emergency room doctor. They are both part of an organization called Doctors and Nurses for Planetary Health, formed in the wake of the 2021 devastation.
In 2021, British Columbia spent late June suffering under a “heat dome”. Temperatures regularly reached 50 degrees Celsius, and by July 1st almost 500 wildfires were burning across the province, including the one that destroyed the town of Lytton. In Nelson, in the Kootenay region, psychologist Dr. Todd Kettner was living with his wife and children in a new housing community with a small ecological footprint. The day after the final home in that community was occupied, a fire sprang up a kilometre away. These eco-friendly buildings were now occupied by anxious homeowners as embers from the nearby fire landed on their brand new roofs.
At the Kootenay Medical Centre in Nelson, Emergency Room department head Dr. Kyle Merritt was seeing patients come in presenting symptoms associated with the wildfire smoke and the heat dome. Acute cardiac events are more common when there is wildfire smoke in the area, and other health issues can become more severe with intense heat. The hospital was not overwhelmed, but there was enough of a concern for Dr. Merritt to take an additional step – and to make headlines doing so.
“I met a patient who had to be admitted because of the heat during the dome. So I made a note, the way all doctors do, indicating what’s going on when you see someone, and in my note I indicated climate change as the underlying cause. The same way you’d say a person was a smoker all their life and now they have lung cancer. You don’t diagnose someone with smoking cigarettes, you diagnose them with lung cancer – but you might write down use of tobacco as the underlying cause.”
This move caused something of a sensation, as newspapers both locally and globally picked up the story of a doctor who had diagnosed a patient with Climate Change. Of course, this was not really what Dr. Merritt had done. One cannot be “diagnosed” with Climate Change, and listing the underlying cause is not the same as the diagnosis. But a clickbait headline remains a powerful force in our society, and the story spread like mint in my garden.
Author’s note - it might be time for us to update our idioms when it comes to the speed with which something spreads. Right now, almost all of those sayings involve either pandemic-type diseases or wildfire. It seems like the wrong phrase to use given the fact that we are still dealing with a global pandemic that has killed millions, and in this case are talking about wildfires that displaced thousands and caused several deaths of their own. And so I humbly suggest “spreads like mint in my garden”. Let’s make it happen!
The heat, the fires, and the devastating problems they caused prompted Dr. Merritt to join some colleagues in creating an organization called Doctors and Nurses for Planetary Health (DNPH). Health care professionals were seeing the direct effects of climate change on the health of the people they served, and thought they could do more. Since then the organization has expanded to include healthcare professionals of all kinds, including Dr. Kettner. They are a lobbying group, an advisory body, and a collective dedicated to making the fight against climate change a central part of their own practices in and around Nelson, B.C.
Nelson is a small city / large town in the Kootenays, with a population of about 10,000 and deep roots in the resource sector. Founded as a mining town 130 years ago, and maintaining strong ties to the forestry industry today, Nelson residents tend to feel a connection to the land around them in the way many small towns with picturesque surroundings do. Combine that with the influx of young, mostly liberal, Americans evading the Vietnam draft in the late sixties and you have the kind of town where establishing a collective like Doctors and Nurses for Planetary Health is a little easier than it might be elsewhere. As Dr. Kettner puts it, Nelson is going on “50 years of hippie-hood”.
Author’s second note – I really wanted to name this piece ’50 years of hippie-hood’ because I love the turn of phrase. I even promised, when I heard it, that I would do so. But I reconsidered at the last moment, because I am reticent to reinforce the harmful stereotype that climate action, and caring about environmental issues, is something ethereal that is solely the domain of aging hippies and young punk musicians. It is, of course, something that affects us all and something that people care about in all walks of life and across all cultural boundaries.
While the members of DNPH are environmental activists of one kind or another, it’s their position as healthcare providers that imbues their message with an authoritative tone. Dr. Kettner says “when we look at who people trust when it comes to the environment, it’s not politicians, or environmental activists or loggers or miners, it’s often healthcare professionals - nurses, or their family doctors.”
We’ve seen, over the past few years, an erosion in trust among the public when it comes to healthcare professionals. People protesting at hospitals, people disrupting life for everyone else over a false belief that the COVID vaccine is somehow responsible for people dying in greater numbers than COVID itself. While those people are the noisiest, they do not represent the majority of Canadians and doctors remain a profession that enjoys overall public trust.
This is especially true in Nelson. Another reason Dr. Merritt and Dr. Kettner and their group are able to produce results is that Nelson really is small. The people you play hockey with on Tuesday nights are the same people you see at the grocery store and the ones who reach out to you for professional help. In Dr. Merritt’s case, that means he has patients who have been under his care their entire lives. For Dr. Kettner, this means his practice and work is integrated into the community he has called home since he started his career as a psychologist nearly 25 years ago. Community connections create strong bonds, the kind that are tough to break. The kind that can weather the storm of online disinformation.
The DNPH group has been very effective in a number of ways (local infrastructure and transportation projects, reducing the footprint of their health system) but perhaps their biggest impact has been in making the connection between planetary health and human health. Recently they worked with the city to increase the delivery of electricity to homes while reducing the amount of fossil fuels in those homes. This not only benefits the environment, it improves the health of the people who are no longer living with emissions within their own walls.
Says Dr. Merritt, “you can’t have human health without a stable climate, healthy air, and healthy water. A lot of people aren’t making that connection all the time, and we try to think about it in everything we do”.
There are a lot of areas in every job where environmentally conscious and sustainable choices can be made. In healthcare-related settings, those choices almost always come with a health benefit as well. In Dr. Merritt’s case, it’s small things like ensuring the batteries used in the hospital are recycled, and bigger things like tackling the problem of anaesthetic gases and inhalers which include hydrofluorocarbons and chlorofluorocarbons that contribute a good deal to climate change.
“One of the advantages I have in working in primary care in a public system is that I get to interact with people from all walks of life, from cradle to grave within my community. It gives me a good opportunity to get to know what they’re going through. And in the emergency department, when events like wildfires or heat happen, it’s the most vulnerable people who are affected. And with mental health too – it’s people who have underlying mental health problems that get acutely exacerbated during these events, and they show up in the ER to compensate. Part of our role is doing advocacy for health, and climate change is now part of that.”
Author’s note number three. Dr. Kettner says that one of the things that keeps climate change top of mind for folks, and gets them to pay attention, is novel news and information. We’ve all heard a lot about polar bears and permafrost and the Great Barrier Reef for some time, and some have tuned out. Something new that might pique the interest of a person when you’re conversing could bring them back into the climate-aware headspace. Something like “hey did you know that anaesthetic gases are a significant contributor to ozone depletion and greenhouse warming?”
For Dr. Kettner, his involvement with organizations like DNPH allows him to share his expertise when it comes to the mental health effects of climate change. His work with the MIR Centre For Peace at Selkirk College has brought an additional lens of intersectionality with the climate crisis. Not only is there a crossover when it comes to health and mental health, there is a significant correlation between climate change and global peace, social justice, and inequality.
“I now feel like I’m focusing on the most important issues – the social determinants of health, greater access to mental health services for greater numbers of people, respect and reconciliation with Indigenous people. It’s where I want to focus a lot of my energy in the last 20 years of my professional career.”
Author’s note number four. While we were discussing Indigenous reconciliation, we spoke about the Haudenosaunee’s Seventh Generation Principle. It’s the philosophy they’ve abided by for hundreds of years, that states you are not only the steward of your environment for yourself and your offspring, but for their offspring and the generation after that and so on. Dr. Merritt shared what I think is an interesting thing to know – either for consideration in Canada or to one day help you win on Jeopardy! There is a new position that was created by the government of Wales in 2015. Sophie Howe completed the first term as Wales’ Future Generations Commissioner in 2023, the role is now held by Derek Walker.
There are several towns in the Kootenay region, and both Dr. Kettner and Dr. Merritt reference a sort of Springfield-Shelbyville type of rivalry between them. But this rivalry quickly disappears when it comes to achieving sustainable practices, and especially in the wake of the recent disastrous climate-related events. Dr. Kettner describes the situation as the wildfires of 2021 were abating.
“Teachers reached out to me from other towns around B.C. looking for resources to help their students with their anxiety when they returned to school after the raging forest fires that had sent them home for a month. That’s the kind of call I didn’t get as a one-on-one private practitioner seeing someone in my office for depression. Expanding our realm of influence to the public as well as to our patients is something I feel very strongly about.”
Stepping outside your immediate job always feels a little bit like a risk. It means doing something that may be outside your comfort zone, and risking a certain amount of venom from those inclined to oppose your initiative who demand you ‘stay in your lane’. It may feel a little less risky in a place like Nelson, B.C., but it still requires a little bit of daring. It’s a testament to the passion both Todd and Kyle feel, and to the immediate necessity of such action, that they have taken that step. And having done so has already made a significant impact.
Their DNPH group has been heavily involved with the city’s new Active Transportation plan, ensuring it is as sustainable and eco-friendly as possible. A number of their doctors and nurses present some of their advancements to neighbouring towns. The group is working with forestry experts on land adjacent to the city to decrease fire risk while increasing access for people to reap the mental health benefits of being able to go for a walk out in the woods. They are now being included in a lot of major decision-making, and their advice is sought on projects that have little to do with healthcare – except for the central thesis of Doctors and Nurses for Planetary Health. That is, that planetary health and human health are inextricably linked.
Author’s final note – while we were speaking, Dr. Kettner reminisced fondly about a series of TV commercials from his youth, which featured the Kokanee glacier in ads for Kokanee beer. He bemoaned the speed at which that glacier is now disappearing, an additional reminder of the devastating effects of climate change right there in their own backyard. In the course of this discussion, we discovered that Kokanee beer remains one of Canada’s best-selling brands to this day. Which surprised me, I didn’t think it was even being brewed any more, at least not since I was in high school and also saw those commercials. I thought that was interesting enough to add to this piece – Kokanee, it seems, has a great deal more staying power than I imagined it did!
Glaciers, sadly, may not have quite so much.

Marjolaine Rivest-Beauregard and Justine Fortin
Montréal psychology students Marjolaine Rivest-Beauregard and Justine Fortin created the podcast Sors de ma tête to combat disinformation and to make science accessible for non-scientists toward the beginning of the COVID-19 pandemic. They joined the CPA podcast Mind Full to discuss their work, which has branched out a little bit as they get ready to launch their third season.
Knowledge translation is a rare skill, not necessarily inherent in most people pursuing a scientific discipline. Being good at knowledge translation means you have to have the knowledge base in your subject matter, but also a communication style that can engage people outside that scientific bubble to want to learn more about that subject. Knowledge translation also requires an ability to take a 10,000-foot view of scientific information. What would regular people like to know? How do I explain this to them while still being as accurate as possible to the source material? What words might I use that would lose my audience, and what seemingly complex terminology and concepts might be grasped intuitively?
One of the best ways for people working in scientific disciplines to become good knowledge translators is – as it is with all skills that can be honed – practice. It was with that in mind that Marjolaine Rivest-Beauregard and Justine Fortin embarked on their passion project – explaining difficult psychological concepts and studies to the general public in an effort to combat online disinformation.
Justine and Marjolaine are about to launch the third season of their French-language podcast Sors De Ma Tête. Montréal psychology students and colleagues, they began this project in 2021 with an eye toward COVID and the disinformation surrounding it. They wanted to collect the data they had on COVID, then sit down with two other people. An expert to talk about the science, and someone with a large public platform to speak directly to people.
Justine is at UQAM, Marjolaine is at McGill, and they met thanks to the supervisor they had in common, Dr. Alain Brunet. Dr. Brunet of course became the first guest on the program (see the CPA’s podcast Mind Full, where the first guest was CEO Dr. Karen Cohen) to discuss the emotional reactions people were having to COVID and to lockdowns. The other guest on their first episode was Instagram content creator Cassandra Bouchard. Cassandra posts funny videos online and speaks about mental health issues – toxic relationships, quitting smoking, eating disorders – that sort of thing.
The process for choosing an online influencer to join Sors de ma tête is probably a more arduous one than the process for choosing the expert. After all, it’s clear who has the expertise in most subject matter – but for people who have a following and discuss mental health issues on their platforms, it’s a little tougher to narrow down who has both the competency and the communication ability to be part of the bridge to the public. Marjolaine says there are a few essential traits each person must have.
- They talk openly and often about mental health
- They are willing to speak openly about their own stories and experiences
- They are available on the day and time the podcast is going to be recorded!
Justine says they also look at the following of the people they invite. She says “we’re not known by people 18-35 years old, so people with large followings are great – our goal is to reach the most people we can”. She also says a lot of this comes down to personality and energy. She tries to find people with similar energy levels who match well in a public discussion like a podcast. Finding the right expert to pair with the right content creator can be a difficult exercise in itself, but can produce some very rewarding content. Says Justine,
“One of my absolute favourite episodes was the last one we did in 2022 [‘Trahison amoureuse avec Michelle Lonergan et Marie Gagné’]. We had so much fun, we were laughing the whole time, talking about betrayals we had lived through, the crushes we had as kids. It’s a bit of a sad subject but the conversation was light and super enjoyable.”
From here, Marjolaine’s main focus is on research. She hopes to get her doctorate degree and pursues research into the mental health effects of disasters and crises, with a focus on prevention. She is imagining a side gig as a crisis management consultant, someone who helps to mobilize the response to a disasters (the earthquake in Turkey, the recent tragedy in Laval) in a scientifically sound and evidence-based way.
Justine’s career path, at least as she sees it from here, is a little different. She is focusing on both research and clinical work, and hopes to one day open a clinic as a neuropsychologist. She really wants to continue working with people who have been diagnosed with cancer, and talks with passion about ‘chemo brain’ and the other issues affecting people in cancer treatment. She want to continue doing research as well, saying “I don’t want to be a professor, as such, but I’d love to keep doing research. Maybe in Marjo’s lab!”
It would be great to think that for years to come, these two partners and collaborators will continue to work together on projects big and small. The third season of Sors de ma tête will launch very soon, and while Justine and Marjolaine are cagey about the content this year, they let slip that climate change will be a big front-and-centre subject in 2023.
It’s unclear right now how long the podcast will last. Will it be a project they keep up until the end of school? The end of COVID? Maybe much longer? Only time will tell. The one thing we can say for certain is that people like Justine and Marjo, the people who have put in the time and the practice, will be the knowledge translators of the future. The people who can bridge the gap between scientists and the public, who can push governments to make decisions based on hard data and otherwise unknown studies. With the Sors de ma tête podcast, they’ve already spent two years doing just that.

Dr. Herman George Canady
Herman George Canady has had a lasting influence on psychology, influencing theories like intergroup anxiety and stereotype threat. He was also one of the very early leaders in organizing a group of Black psychologists.
The current psychological theory of ‘intergroup anxiety’ describes a feeling of discomfort many people feel when interacting with people from groups that are not their own. A lot of that theory owes a great deal to Herman George Canady, whose work looked at Black students interacting with white examiners while taking IQ tests. If the examiner is white, and the Black child has experienced discrimination and prejudice from white people in the past, they are likely to be anxious and perform poorly on the test simply because it is administered by a person whose presence makes them nervous.
Dr. Canady’s study ‘The Effect of ‘Rapport’ on the I.Q.: A New Approach to the Problem of Racial Psychology’ was the first of its kind to look at intelligence tests through this lens and led to many further studies examining the effect of a distrust of White people on the test scores of Black children. In many ways, Canady was one of the first psychologists to focus research on the Black experience in the United States.
This lack of Black inclusion in research, and a lack of psychological knowledge for Black Americans in general, led Dr. Canady to lead a movement organizing Black psychologists. He wrote A Prospectus of an Organization of Negroes Interested in Psychology and Related Fields and sent it to fellow members of the American Teachers Association (formerly the National Association of Teachers in Colored Schools), proposing a psychology section within the ATA.
Canady presented his proposal at the ATA convention, held at the Tuskegee Institute, in 1938. It was unanimously approved – but then quickly derailed by the onset of World War II. In later years the cause would be taken up again when Black psychologists organized at an APA convention in 1968 to discuss their dissatisfaction with "psychology's exploitations and the white definitions for behavior that placed Blacks in a negative light."
Dr. Canady obtained his B.A., his Master’s, and his Ph.D. from Northwestern University. He later served 40 years as the chair of the psychology department at the West Virginia Collegiate Institute (now West Virginia State College) before his retirement in 1968. He died in 1970, but his influence is still felt in intergroup anxiety research, stereotype threat studies, and in the ongoing effort to move psychology out of a white-centric model.
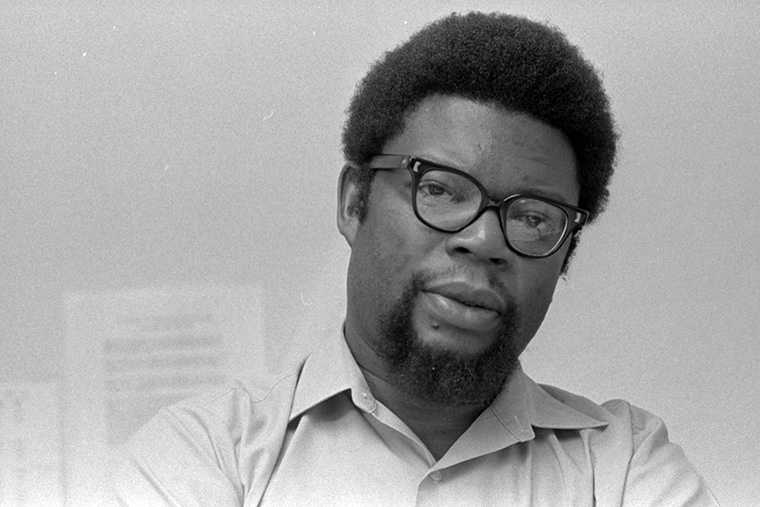
Dr. Robert Lee Williams II
Famous for three important books, and for coining the word ‘Ebonics’, Dr. Robert Lee Williams II spent his long and influential career combatting the racist stereotype that Black people were less intelligent than White people.
“Cars is whips and sneakers is kicks
Money is chips, movies is flicks”
- Big L., ‘Ebonics’
The word ‘Ebonics’ didn’t exist before 1973, when Dr. Robert Lee Williams II took the word ‘ebony’ and the word ‘phonics’, combined the two, and coined a brand new term for “linguistic and paralinguistic features which on a concentric continuum represent the communicative competence of the West African, Caribbean, and United States slave descendants of African origin." His 1975 book Ebonics: The True Language of Black Folks, traced the roots of Ebonics to Africa, arguing against the prevailing prejudiced opinion that Ebonics was just slang, or bad English.
Dr. Williams was born in Arkansas in 1930, and enrolled in Dunbar Junior College at the age of 16. He dropped out after only one year, having become quickly disillusioned upon being asked to take an IQ test. The results of the test suggested he was more suited to manual labour than he was to more intellectual pursuits. While this test had a huge impact on his self-esteem, racial bias in standardized testing later became the driving force behind some of his most important work. In particular, the Black Intelligence Test of Cultural Homogeneity, or BITCH-100, which he created in 1972 to account for the cultural factors affecting Black Americans differently than White Americans.
Dr. Williams obtained his Ph.D in clinical psychology in 1961 from Washington University, and in 1968 was a co-founder of the Association of Black Psychologists, later serving as its second President. The ABP was created as an alternative to the American Psychological Association, which was criticized for intentional and unintentional support of a structurally racist American society. The ABP’s membership saw themselves as “Black people first, psychologists second”.
He went on to found the first department of Black Studies at Washington University, where he worked as a professor of psychology, African studies, and African-American studies from 1970-1992. He continued to maintain a high profile through media appearances supporting his books – 1981’s The Collective Mind: Toward an Afrocentric Theory of Black Personality, 2007’s “Racism Learned at an Early Age through Racial Scripting”, and 2008’s History of the Association of Black Psychologists: Profiles of Outstanding Black Psychologists.
Dr. Williams was married to his wife, Ava Kemp, for 70 years until she died in 2018. He passed away in 2020 at the age of 90. He had eight children, four of whom went on to become psychologists.

Nardeen Yalda
Our podcast Mind Full spoke with Nardeen Yalda and her professor at the University of Western Ontario, Dr. Leora Swartzman. Dr. Swartzman has created a program to pair students with community organizations to implement change on the ground. That program led Nardeen to working with organizations helping the homeless.

Dr. Ruth Winifred Howard
One of the first Black women to earn a Ph.D. in psychology, Ruth Winifred Howard trained Black nurses and worked with children and youth during her long and exemplary career.
There is some debate as to who was the first Black woman to obtain a Ph.D. in psychology. Some say it was Inez Beverly Prosser, who received her Ph.D. in 1933 from the University of Cincinnati. Others think it was Ruth Winifred Howard, since they consider a psychology Ph.D. to count only if it comes from a psychology program – she graduated in 1934 with a doctorate in psychology and child development from the University of Minnesota. There is no record of whether either woman cared at all about the distinction.
Ruth Winifred Howard was born in 1900 in Washington D.C. Her father was the minister at the Zion Baptist Church and was heavily involved in many community initiatives. Ruth would later say this example was what led her to desire a career helping others, and led her on the path to becoming a psychologist. That path began at Simmons College in Boston, where she majored in social work and earned a Bachelor’s Degree in 1921. It ended at the University of Minnesota, where she obtained her psychology Ph.D. 13 years later.
For her doctoral research, Dr. Howard studied triplets. Specifically, she launched the most comprehensive study ever done on triplets, studying more than 200 sets ranging in age from birth to their 70s. For reasons yet unknown, it took more than a decade for that research to be published, in 1946 in the Journal of Psychology and in 1947 in the Journal of Genetic Psychology. By then, she had married fellow psychologist Albert Sidney Beckham and moved to Chicago.
With her husband, Dr. Howard opened a private practice where she worked with children and youth, while working as a psychologist at the dated and terribly-named McKinley Center for Retarded Children. She was also the staff psychologist at the Provident Hospital School of Nursing, training Black nurses, and was a psychologist for the Chicago Board of Health until 1972.
In 1964, Ruth’s husband Albert died. She kept working for a few more years, both in private practice and with the Chicago Board of Health. Dr. Ruth Winifred Howard died in 1997, just a few days shy of her 97th birthday, having left an important legacy. More than just a pioneer, paving the way for others to follow in her footsteps, Dr. Howard’s work made a marked difference in the lives of hundreds of children in Chicago and around the world.
Nancy Tangon
Nancy Tangon is a CPA student representative at the University of Alberta. Her South Sudanese family has played an enormous influence in her life, including her decision to pursue a career in psychology.
With her friend Priscilla Ojomu, Nancy created the online forum Canada Confesses, where they collect anonymous testimonials from people that shine a light on the racism that exists under the surface in Canadian society. They spoke with the CPA podcast Mind Full about their project. https://soundcloud.com/user-389503679/mindful-9-canada-confesses-01162023-mixdown-1/s-Y9IhuOvB5gY
“We did a three-hour boot camp over Zoom about how to create a presentation and become a better public speaker.”
The first lesson, when it comes to creating a presentation, is not to make that presentation three hours long. A boot camp though? That can be as long as you like. In this case, Nancy Tangon and her CPA Student Representative colleagues at the University of Alberta chose the boot-camp format – and the Zoom format – out of necessity. Because of the pandemic, many things have become more difficult. Finding ways to connect with people virtually has resulted in a fair amount of chaos – and a ton of creativity as well!
Such was the case when Nancy and her fellow student Priscilla Ojomu were looking to create a project. Pre-pandemic, they met in On-Site Placement’s Diversity Awareness & Skill Building Youth Program on campus – in-person, if you can remember when we used to do such things! Through that program they learned a lot about issues affecting diversity in a number of settings, and were tasked with creating a project at the end of the course. Unfortunately, by that time COVID-19 had arrived and the project would have to take a virtual form.
Over the course of the pandemic awareness of many issues has increased – particularly those dealing with discrimination and inequality. In Canada, many of us felt isolated from those issues – like they were a uniquely American thing, or that we were somehow better off. As Priscilla says, “a lot of Canadians aren’t aware that these issues exist in huge numbers within Canada”. So how could she and Nancy help to increase that awareness?
Their answer was Canada Confesses. A project that started out small but has since taken on a much larger audience and significance. The concept was simple. There’s a disconnect between what Nancy and Priscilla learned in their program, as well as their own lived experiences, and what fellow Canadians understood to be the situation. So they created a place where marginalized people could tell their stories anonymously, access resources to help them, and help other Canadians understand the reality of what’s happening in our country. It’s not the anonymous poster who is confessing, although they call the posts ‘confessions’ – it’s Canada itself that is confessing to the ongoing harms and structural marginalization of many communities. You can hear all about Canada Confesses on the CPA podcast Mind Full.
As the co-creator of Canada Confesses, Nancy has not yet submitted a ‘confession’ of her own – she’s very busy! In addition to running a suddenly successful online platform which continues to grow by leaps and bounds, she is also a fourth-year psychology major and biological sciences minor at the University of Alberta. She maintains a strong presence in the CPA, with two years as a Student Representative on the campus and a significant role on the CPA’s human rights and social justice committee as one of the leaders of the subgroup for ableism and disabilities.
“I was a little bit intimidated to [join the Human Rights and Social Justice committee]. Everybody who’s a part of it is either a grad student or a professor, and at first I felt a bit like the undergrad student tagging along. But it’s been really great! I got to learn a lot from Dr. Ada Sinacore and Dr. Laurie Ford, who’s also a part of our subcommittee.”
Nancy, undergrad or not, brings a lot of experience to the CPA board committee – and to her life, her studies, and her activities. Much of this stems from her family and her community, with whom she is very close. Her family on her father’s side is from the Bari tribe in South Sudan, a place Nancy has been able to visit only once. She keeps up contact and correspondence with her family who remain there, and also maintains strong ties to the South Sudanese community in Edmonton.
“The South Sudanese community in Edmonton is fairly large, I know a lot of people here – especially compared to when my family used to live in Halifax. I even see some of the community members in my classes, which is really cool. When I decided to go to university, I wanted to do something amazing in my community. In the South Sudanese community, psychology is very interesting to a lot of people.”
Her family, and her community, were some of the factors that shaped Nancy’s desire to go into psychology in the first place – and even had a guiding hand in deciding on some of the courses she took once she got there. Nancy’s family loves to talk about their dreams. She says, “when I wake up I have to talk about my dreams. I talk about it to at least five people before I start my day! I have to analyze it just a little bit, I have to get someone else’s interpretation, and I absolutely love dream analysis.” Of course, she felt she just had to take that particular psychology course before she graduated, and now speaks excitedly about the ‘subjective’ and ‘objective’ levels of dream analysis.
It didn’t take long for Nancy to determine that psychology was the right program for her – or in which direction she wanted to go with it.
“I was inspired by my very first professor on my very first day. Her name is Dr. Peggy St-Jacques. She was pretty new to the university at the time, and she was doing research in memory. I said, I don’t know exactly what I want to research, but that is certainly what I want to do as a lifelong career.”
Nancy is now well on her way, working as a research assistant and planning for a future where research is part of her every day. She’s particularly drawn to developmental psychology, and hopes to work with pre-school children between the ages of three and five. It will be a long road, but Nancy has the determination, the ingenuity and the curiosity to make it a successful one. And when she does, it will be another in a long line of successes that started right there in Edmonton.
“When I started working on Canada Confesses, it was almost impossible to see where we would end up. I’ve had the chance to meet so many people working in the same field, and to interact with other projects online. Now, I have a best friend for life, an amazing team, and so many things to anticipate for the future.”

Kevin Prada
Kevin Prada is a student at the University of Manitoba, where his research focuses on the difficulties faced by the French-speaking 2SLGBTQ+ community in Manitoba.
Kevin and his colleagues, including Thilini Dissanayake, started an initiative in their area called A Listening Ear. They joined the CPA podcast Mind Full to explain the project. https://soundcloud.com/user-389503679/psychology-month-kevin-prada-and-thilini-dissanayake-lend-a-listening-ear/s-Ze0rXFQvsaN
“French is a pretty binary language. It’s something you maybe don’t think about, but how do you become gender-neutral in a language that depends so heavily on a gender-binary?”
We hear a lot about ‘intersectionality’ these days, referring to the way social categorizations interplay with one another. An individual, or a group, can be connected to others based on their race, their sexuality, their gender, or their socio-economic status, among myriad further distinct, yet inextricable identities. As such, each person’s identity is unique, but each connects, intersects, and overlaps with others, leading to unique forms of oppression or stigmatization for some, privilege for others, or a mix of both for others still.
Such is the case for all of us, but few of us are as keenly self-aware of such intersectionality as is Kevin Prada – both personally and in his research. Kevin is a student in the psychology honours program at the University of Manitoba. A queer Franco-Manitoban, Kevin has long seen the gaps in the Manitoba mental health system for both the 2SLGBTQ+ community and the French-speaking community. This led him to collaborate on his first major research project[i], one that earned him the Ken Bowers Student Research Award from the CPA’s Clinical Psychology Section.
His research focused on both of those identities – 2SLGBTQ+ communities and official language minority communities in Manitoba. In the first study of its kind in Western Canada, Kevin and his colleagues launched an exploratory analysis into the needs of doubly-minoritized French-speaking 2SLGBTQ+ Manitobans. Initiated by the Collectif LGBTQ du Manitoba, whose first mandate was to collect data about the needs of this very specific community, this community-based project was conducted by researchers at Université de Saint-Boniface.
“Before we start doing anything for a community we’d better understand where they’re at, what their needs are, and what their experiences are in terms of discrimination and stigmatization. We know that minority Francophone populations in Manitoba have lower indicators of health than the general population. We know similar trends have been observed across the board with queer populations in Canada and abroad. When the two identities are put together, it stands to reason that those problems probably compound.”
This has always been planned as a multi-tiered research project. Kevin and his colleagues have completed Phase One, surveying 80 respondents over the age of 18. Phases Two and Three have already begun, focusing on school and family contexts, to determine both the needs of queer and questioning Francophone minors in school settings, and also to examine the transition to parenthood for queer families in an official language minority context. This has led to many opportunities for Kevin to speak at professional development days for Francophone and French-immersion schools and school districts, where he says,
“Many staff are ready and willing, and want to build proactively queer-friendly classrooms, but don’t always know where to start. Invaluable questions and discussions have ensued, which show me how important it is to discus these sometimes-complex issues with folks in an open and non-threatening way, especially with an eye toward the potential implications within school environments.”
When intersectionality is approached in the right way, there is often a ripple effect – sometimes one that is by design, sometimes an unintended one that comes as a surprise. For Kevin, these ripple effects have been overwhelmingly positive, affirming, and a reinforcement of the direction he wants his career to take.
“We now have folks in Alberta and elsewhere who are starting with our research project to create their own in their own province. So the impact has been even greater than we’d expected. And for myself, as a queer Franco-Manitoban student and researcher, to be able to have done this for my community was really life-giving. We also really put an emphasis on ensuring that this would be by the community, for the community, and from the community. Not only were community members involved at every step (myself included), but they were also the first to hear what we found. We conducted two community engagement meetings where only people from our community were invited. Following one of these, one participant emotionally shared that ‘this is what we’ve known and been saying for decades – now our experience is reflected in that data’. It was kind of a cathartic experience for a lot of people.”
Kevin’s big goal, overall, is to work with minority communities. To ‘hear the unheard and see the unseen’, as he puts it. This feels like a personal mantra to him, the kind of thing he says to himself before starting a project or taking the next step. The kind of thing that he will one day have embroidered and framed and placed on the wall across from his desk as a constant reminder of why he’s doing what he does.
“Using intersectionality as one of the major frameworks for this study was really important. Understanding that a French-speaking queer person cannot be understood by just looking at their Francophone identity, or just by looking at their sexual or gender diversity. It’s ‘both-and’. Those two identities AND their age, AND their socioeconomic status, AND their health, whether they are a visible minority, the list goes on. In fact, we found there was a fairly large group of respondents who felt welcome neither by the French-speaking community because of their sexual orientation or gender identity, OR by the 2SLGBTQ+ community in Manitoba because they’re French-speaking.”
Of course, there are many language minorities in Manitoba besides French. In a project completely unrelated to this research, Kevin and his colleagues Saeid Maghsoudi, Thilini Dissanayake, and Aman Mir started an initiative called ‘A Listening Ear’, where they set up booths around Winnipeg to converse with complete strangers in NINE different languages – enticing them to stop for a chat by displaying, for example, a Sri Lankan flag. The effort was a tremendous success, and you can hear more about it on the CPA’s podcast Mind Full.
This is the kind of outreach Kevin is making his brand. He felt first-hand, from a young age, how important reaching out could be and how lonely life could be when no one extends that hand. This is one of the reasons he chose psychology as a career path.
“I grew up in a home that had fairly significant psychological obstacles, especially with my mother. I saw a failure in the system when I was just this little boy who nobody bothered to ask ‘hey, how are you doing?’ In my household, there were multiple suicide attempts, manic episodes, and through it all nobody took a step back and said, ‘oh my God there’s an 8-year-old boy here – is HE okay?’ In retrospect, I saw all this and figured if I went through it I’m sure I’m not the only one. So my first desire to get into psychology was to kind of make sure that the collateral impact of mental health issues is top of mind, especially in families who might be struggling with issues of this nature.”
As he grew up, he saw more and more failures in that system – for 2SLGBTQ+ youth, for Francophone communities, and especially for those like him who lived at the intersection of the two.
“I never had a chance to speak to a queer person growing up, never mind a queer psychologist. The first time I ever met a queer counselor was a huge experience for me, and I only got to access this support when I was 27. So to be able to do something for a marginalized community, especially within the psych discipline which has historically not been super-friendly with queer folk, is exciting.”
Kevin’s ultimate goal is clinical work, where he can meet people, get to know them, and offer culturally competent clinical support. He does not know of any practicing French-speaking clinical psychologists in Manitoba, has not encountered any openly practicing queer clinical psychologists in his province, and highlights the extreme difficulties in the province just obtaining information on queer physical and sexual health in French. There is definitely a lack of representation and, as his research demonstrates, a need for more culturally competent services in Kevin’s immediate area. He wants to be one of the first to provide those services.
“With the right tools, mindset, and adequate understanding of trauma and minority stress, anyone can be a good clinical psychologist with a queer person. But it brings it to another level when you’re actually speaking from a place of personal experience.”
The French language, just by the nature of the language itself, makes some communication difficult for the 2SLGBTQ+ community. When even a table, or a propellor plane, or a block of cheese are assigned either a masculine or a feminine gender, it can create a bigger hill to climb for those people who identify as neither. In English, we use ‘they’ as a pronoun that can be understood by everyone. In French, they’ve proposed brand new pronouns, with ‘iel / iels’ being the most commonly used. However, to this day those new words have still not been officially accepted by the Académie Française.
Understanding our unique identity through an intersectional lens can be an empowering or disenfranchising, oppressive or uplifting, confusing or clarifying journey. In many cases, it is all of these things. Navigating those waters is no easy task, especially for those whose intersecting identities are both marginalized and in conflict with one another. Kevin’s personal experience, his direct involvement in affected communities, and his mantra - ‘hear the unheard and see the unseen’ – make him well-suited, and well-equipped, to be on the vanguard of the change Manitoba so desperately needs.
[i] Living in a liminal space: Experiences of 2SLGBTQ + official language minority Canadians during the COVID-19 pandemic

Dr. Francis Cecil Sumner
The first Black person to earn a Ph.D. in psychology, Francis Cecil Sumner spent his career working to elevate African-American education through more funding and more teaching of Black history.
The first Black person to receive a Ph.D in psychology, Francis Sumner was born in Arkansas in 1895. His parents worried about the quality of the education young Francis was receiving at his local elementary school, and so they taught him at home from what books they had available. When he applied to Lincoln College, a historically black university now known as Lincoln University, his application cited ‘private instruction in secondary subjects by father’ as he did not have a high school diploma.
Dr. Sumner passed the entrance exam and began his schooling at Lincoln at the age of 15. At 19, he graduated as valedictorian with a degree in philosophy. He moved on to Clark University for a second bachelor’s degree, where he became part of a mentor-mentee relationship with then-President of Clark, the pioneering psychologist G. Stanley Hall.
Sumner was drafted into the US military in 1918 and served in Germany in World War I before returning to Clark to complete his doctorate in 1920. Then, as now, psychological science was very Eurocentric, and Dr. Sumner focused on dismantling the racism and bias influenced by that Eurocentrism. Specifically, the studies at the time that purported to show intellectual inferiority in African-Americans. He tackled inequality in the judicial system and unequal outcomes in mental health between people of different races.
In 1939, his application for membership in the Southern Society for Philosophy and Psychology was rejected, after the SSPP changed its bylaws for the express purpose of excluding a Black member. Other members of the society threatened to resign if Dr. Sumner was not accepted, and his application was eventually improved, with the leadership of the society blaming a secretary.
From 1928 until his death, Dr. Sumner served as the chair of the psychology department at Howard University, a historically Black research university in Washington D.C. While there, he taught many Black psychology students including Kenneth Bancroft Clark, an influential leader in the civil rights movement and the first Black president of the American Psychological Association.
Dr. Sumner’s legacy endures to this day, as his lifelong efforts to elevate African-American education through more funding and more teaching of Black history and the Black experience have influenced modern education in many ways. Upon his death, he was memorialized with tributes of all kinds, including some that referred to him as ‘Howard’s most stimulating scholar’ and others that called him the ‘Father of Black Psychology’.

Sam Ayers-Glassey

Naya Goguen
For many students in the CPA Student Section Mentorship Program, the most valuable advice a mentor can provide is around applying to grad school. For Naya Goguen, the most valuable advice she got from Sam Ayers-Glassey was quite the opposite.

Maya Atlas

Kiana Chubey
Mentor Maya Atlas nominated her mentee Kiana Chubey for Student Section Mentorship Program Mentee of the Year. Although their paths to studying psychology were vastly different, the two have a strong connection based on similar goals.

Linnea Kalchos
Linnea Kalchos is the new Chair of the Student Section of the CPA. She is hoping to continue, and expand upon, the Student Section’s legacy of social justice work.

Kayla Hollett

Liran Leidershnaider
Kayla Hollett has been a mentor in the CPA Student Section Mentorship Program for a while, and this year nominated her mentee Liran Leidershnaider for the Mentee of the Year Award. Their connection is strengthened by the virtual platform with which they interact.

Stephanie Woolridge

Ava Homiar
Stephanie Woolridge was the runner-up for the CPA Student Section’s Mentor of the Year award. Her connection with mentee Ava Homiar is profound, and goes much deeper than just academics.
We speak with members of the Sexual Orientation and Gender Identity section about issues facing the LGBTQ+ community during the pandemic, the history of the fight for marriage equality and the more recent effort to ban conversion therapy. We also learn a new term: ‘Femmephobia’.

Dr. Steve Joordens gave his first-year psychology class a group project – bust some myths around homelessness by collaborating with a local organization. Zaynab Azeem was inspired to work with Blankets for TO, and has turned that inspiration into a podcast of her own!

Dr. Meghan McMurtry joins Mind Full to talk about needle fears, needle pain, and coping strategies for all of us who experience one or the other. This includes advice about vaccinating infants and very young children.
Dr. Houyuan Luo joins Mind Full to talk about his own struggles during the pandemic, and how he tries to avoid burnout. We also discuss options for people who are able to access therapy, and for those who can not.
Dr. Stryker Calvez and Dr. David Danto talk Truth, Reconciliation, and the role of Psychology from the perspective of an Indigenous psychologist and an ally. We discuss Indigenous ways of knowing and how the apply to psychology, as well as the genocide perpetrated by Canadians against our Indigenous people.

Dr. Jesse Bosse is a gender-queer psychologist in Ottawa who works primarily with trans, non-binary, and gender-diverse people. Aida is a young trans person who is currently undergoing Hormone Replacement Therapy. We spoke to them both about the issues confronting gender diverse people, human rights issues, and the effects of the pandemic on this population.”

Dr. Ada Sinacore is an expert in human rights issues surrounding gender diversity. Dr. Keira Stockdale is an expert in the psychology of criminal justice. They are part of a group working to put out a statement on gender diversity amid an increase in violence and legislation targeted at the gender diverse community. We discuss LGBTQ2s+ rights in relation to education, the criminal justice system, and the discipline of psychology itself.

Canadian Indigenous Artist Betty Albert has created a design for a T-shirt that the CPA sold at the 83rd annual convention in Calgary. All proceeds went to an Indigenous charity working towards healing for Indigenous communities in Canada. We discuss art, residential schools, and the remarkable capabilities of Photoshop!
 Drs. Karen Dyck and Melissa Tiessen started the Intentional Therapist initiative to help female practitioners with self-care. They will be hosting a pre-convention workshop at the 2022 CPA Convention in Calgary.
Drs. Karen Dyck and Melissa Tiessen started the Intentional Therapist initiative to help female practitioners with self-care. They will be hosting a pre-convention workshop at the 2022 CPA Convention in Calgary.
Intentional Therapist
It was September 2007 and Melissa Tiessen had just begun her year long post-doctoral residency with the University of Manitoba’s Rural and Northern Psychology Programme, where her primary supervisor was Dr. Karen Dyck. Melissa was no stranger to rural and northern living, as she grew up in a northern Manitoba community. Karen was one of the first psychologists hired into the Rural and Northern Psychology Programme in 1997. Although Karen wasn’t raised in a rural or northern community, she was from Manitoba, and her interest in rural and northern psychology came about during the completion of her doctoral degree in clinical psychology at the University of South Dakota; a program that specialized in community and cross-cultural psychology. Little did Melissa and Karen know at the time, that this would be only the start of a long-term relationship that would move from supervisor-supervisee, to colleagues, to friends, and eventually to co-founders of Intentional Therapist.
During the 15-year span of their relationship, Dr. Melissa Tiessen and Dr. Karen Dyck shared many professional experiences, from working within the public health system in rural Manitoba to eventually moving to private practice. Although Melissa left Manitoba in 2010, they continued to connect with one another and have in-person visits when their travels took them to similar locations. It was during one of these visits in Manitoba in 2018, when Melissa and Karen began discussing self-care, burnout, and many of the issues affecting psychologists and other mental health professionals. Having worked in both the public and private healthcare systems, they observed and experienced firsthand, some of the challenges mental health professionals can experience related to self-care. They reflected on how these challenges can be similar across all mental health professionals but that there may also be some unique challenges related, for example, to the work setting (e.g., rural and northern mental health clinicians may experience equally impactful but different challenges than their urban counterparts) and gender.
And so it was that Melissa and Karen came up with the idea of The Intentional Therapist, an online community that provides resources, workshops, newsletters, and – most importantly – connections to other female mental health professionals. The reason they chose to focus on female practitioners specifically is that, in addition to the pressures and stresses that affect all mental health professionals, women face a few extra hurdles. Melissa explains,
“The biggest factor that affects female mental health professionals in terms of self-care challenges is gender socialization. Many women grow up from the day they’re born being exposed to different messages than those who identify as male. These messages are very much about taking care of others, doing for others, and prioritizing others. Sometimes it can be good to put others’ needs before your own, but that can create a scenario where a girl becomes a woman and goes into a care-taking profession. She has been receiving these messages about taking care of others in her personal life, and now it is part of her professional life as well. It can then become very difficult to do what one needs to take care of oneself.”
This gender socialization has become even more scrutinized during the past two years during the pandemic. Women, including those with high-paying professional careers, have often found themselves taking on more archaic gender roles. The work of men has, in many cases, become more prioritized while the work of women becomes diminished in order to take on caregiving roles for children or elderly parents.
Karen is a caregiver to elderly parents as well as a clinical psychologist in private practice in Oakbank, Manitoba. She says that work and caregiving are not the only places where there is a discrepancy. Leisure time for women has also, historically, been tied to their partner’s leisure time. As men’s status and income improved, they had more access to leisure. Women’s leisure then became tied to that of their partner, and they were often not entitled to their own spare time on their own terms. Leisure activities being so important for self-care, this can make taking time for oneself even more difficult.
So what does that self-care look like? For Karen and Melissa it comes down to the four C’s. The first is ‘connection’ (like the network of like-minded mental health professionals that form the Intentional Therapist). The second is ‘compassion’ (toward oneself, toward your clients). The third is ‘courage’ (meaning doing something that may cause you discomfort). For many mental health professionals, any discussion around money can feel awkward. But raising your fees, for example, might be a necessity. Having that initial uncomfortable conversation can make future conversations of a similar nature much easier.
The final C is ‘creativity’. As Karen says, self-care involves a lot more than just chocolates and a bubble bath. Creativity and a playful attitude can help people find humour in their every day lives and discover activities that help them cope. These activities, and this outlook, is different from person to person. While Karen and Melissa happen to share a love for cake decorating, that certainly isn’t the case for everyone.
For some it might be running, for others painting, and for others it may be weaving plastic bags into doormats (like Melissa did during the pandemic). The important thing is that self-care is intentional. That it is made a priority, and that it remains important day in and day out. Hence The ‘Intentional’ Therapist. Melissa and Karen’s initiative is meant to be pro-active, to reach practitioners before they start to see the symptoms of burnout. Their newsletter, workshops (including a pre-convention workshop at this year’s CPA Convention), and network of female mental health professionals is intended to serve as a kind of regular reminder. You are important too – and in order to provide great care for your clients, you must also take great care of yourself.
Psychology Month Profile: Dr. Charlene Senn and Dr. Lorraine Radtke, Section on Women And Psychology

Dr. Charlene Senn

Dr. Lorraine Radtke
Dr. Charlene Senn, and Dr. Lorraine Radtke, Section on Women And Psychology
The CPA’s Section for Women And Psychology (SWAP) creates a community of researchers, teachers, and practitioners interested in the psychology of women and feminist psychology. Today’s Psychology Month feature talks to Dr. Lorraine Radtke and Dr. Charlene Senn about the work they’re doing in this space.
SWAP (Section for Women and Psychology)
The year is 1976. Martha Lear has just coined the term ‘second wave feminism’ in New York Magazine, and that movement is in full swing. In the United States, Title IX has just passed, prohibiting sex-based discrimination at any school that receives federal funding. In Sweden, Group 8 has just been founded, advocating for equal pay, kindergarten expansion, and a 6-hour work day. And in Canada, the CPA is hosting their annual convention at a hotel in Montreal.
There is a different hotel across the street from the CPA convention. While that hotel is unaffiliated with the one where the convention is taking place, the two are connected by an underground tunnel beneath the street. While the convention is in full swing, many women are stealing away, passing quietly through that tunnel to have a clandestine meeting of their own just across the street. These graduate students and untenured feminist researchers are there to present papers - to one another. These papers are on topics relevant to the psychology of women and girls, and they have one more thing in common. When they were submitted to the CPA for inclusion in the convention, they had all been summarily rejected.
This off-site, convention-adjacent meeting became known as the Underground Symposium. Not so much because it was clandestine – there was in fact a fair amount of media attention – but more likely because it was accessed through that underground tunnel between the two hotels. The event was a huge success, where ideas were flowing and the room was overflowing. It was that success that led, four years later, to the designation of an “interest group” known as “on Women And Psychology”. This later became the Section for Women and Psychology, or SWAP – and that is where we are today.
Members of SWAP need not identify themselves as feminist scholars, but many still do. Section chair Dr. Lorraine Radtke certainly maintains the tradition of that origin story. Dr. Radtke is a professor emerita in the department of psychology at the University of Calgary, where she worked for close to 40 years. She says,
“I identify as a feminist psychologist. It’s because I put women and girls first, and I take a critical perspective when it comes to the status quo. I’m focused on social change and improving the lives of women and girls.”
Feminist psychology has changed over the years. One of the biggest ways it has changed is that research and clinical practice is now conducted in an intersectional framework. This means being open to both the commonalities and the differences among women and girls. It also means being attuned to how their social circumstances such as gender, ethnicity, sexuality, and socioeconomic situation affect their experiences. Dr. Charlene Senn is a professor at the University of Windsor affiliated with the Applied Social Psychology program, and she says her research, and that of her colleagues is always conscious of that intersectional framework. She also says that the study of women and psychology is a broader topic than many may think.
“I am a feminist social psychologist – the distinction I feel is important because psychology is seen as being individual, when in fact it’s also concerned with environmental, cultural, and social forces. I teach a graduate course on feminist psychology and the psychology of women and gender. We look at the tremendous work being done by feminist psychologists in so many different fields, where psychology is being transformed by the work that’s happening in those areas.”
SWAP was not limited from the beginning to feminist psychologists, and today has a membership that involves researchers across all fields, students from various departments across Canada, and clinical psychologists, some of whom work primarily with women and girls. Says Dr. Senn,
“Parallel to feminist work, or work related to women and girls, there is feminist research on a variety of topics - masculinities, for example, and a thread of research also looking at the status of women in psychology, looking at things like inequalities in the field. So there is a real variety.”
Dr. Radtke agrees, and says that this kind of wide variety of work from the lens of women and girls’ psychology forms a big part of SWAP’s history.
“In the early years, members of SWAP were very active in the CPA and other professional associations in Canada, pressing for gender equality and for women to be involved. They advocated for changes to ethical standards that would incorporate a sensitivity toward the concerns of women and girls. It has always had an activist side, and to this day SWAP has a Status Of Women Committee to ensure that all genders and all sexes have equality within the discipline and that those standards continue to be upheld.”
It’s because of the broad approach and diverse membership of both the SWAP section and the Status of Women Committee that they were able to collaborate with the Indigenous Peoples’ Psychology section, the Student section, and the Rural and Northern Psychology section to organize a virtual panel at the 2021 CPA Convention to address the findings of the final report of the National Inquiry on Missing and Murdered Indigenous Women and Girls, and the implications for psychology in Canada. Says Dr. Radtke,
“It was a big collaboration, and very successful. It was decided that they would follow up that panel with a report not only on the panel itself but also with some recommendations. It’s quite an undertaking for a relatively small committee, and they’ll be focused on that in the coming year.” Editor note – as this will be published in February, check back to see if the report has been sent out by then, include an update if it has.
The panel discussion on Missing and Murdered Indigenous Women was a central event at CPA 2021, no one had to sneak across the street to have their voices heard. Dr. Radtke points out that progress has been made both in the discipline and in the organization itself.
“Obviously CPA has become more egalitarian. We’ve seen more women presidents of CPA, we see more women serving on the Board of Directors than was historically the case. Although these problems are less significant in current times, there are still a few issues that require attention, for example, the nomination of more distinguished women for CPA awards.”
These issues will never disappear altogether, and there is a lot more work to do for the members of SWAP and psychologists who work in this space. During the pandemic, the jobs of husbands have taken precedence over the jobs of wives – even when the wife is an academic, even when she out-earns her husband – as childcare is still seen too often from a traditionally patriarchal lens. Instances of violence against women continue to rise as too many are trapped at home with their abuser. Dr. Senn’s specialty is campus sexual violence prevention, and she says that when campuses reopen the rates of sexual assault will likely go right back to pre-pandemic levels. In fact, they have not declined since the 1980s.
The field has come a long way since the Underground Symposium, but getting their work acknowledged remains a work in progress. Dr. Senn says, “we still have to push to have the knowledge we have from the incredible research being done by feminist psychologists incorporated more into the mainstream.” She pauses and exchanges a knowing glance with Dr. Radtke. “Including intro To Psych textbooks.”