
Psychology Month has focused on dozens of aspects of the pandemic, a global catastrophe that is deeply tragic. To close out Psychology Month 2021, we focus on a few positives that have come about as a result of COVID-19.
Month: February 2021
Psychology Month Profile: Karen Cohen
 Dr. Karen Cohen
Dr. Karen CohenPsychology Month Profile: Dr. Jenn, Dr. Laila, Dr. Mary and the Coping Toolbox podcast
 Dr. Jenn, Dr. Laila, and Dr. Mary
Dr. Jenn, Dr. Laila, and Dr. MaryFriends since they did an internship together at the Children’s Hospital of Eastern Ontario, child psychologists Dr. Laila Din Osmun, Dr. Mary Simmering McDonald, and Dr. Jenn Vriend are trying to reach as many kids and parents as they can during the pandemic with the Coping Toolbox podcast.



Psychology Month – Dr. Jenn, Dr. Laila, Dr. Mary and the Coping Toolbox podcast
 Dr. Jenn, Dr. Laila, Dr. Mary and the Coping Toolbox podcast
Dr. Jenn, Dr. Laila, Dr. Mary and the Coping Toolbox podcast
Introducing The Coping Toolbox: A Child Psych Podcast. Dr. Jenn Vriend, Dr. Laila Din Osmun, and Dr. Mary Simmering McDonald are three child psychologists from Ottawa.
https://podcasts.apple.com/ca/podcast/the-coping-toolbox-a-child-psych-podcast/id1553993639
Black History Month: Charles Henry Turner
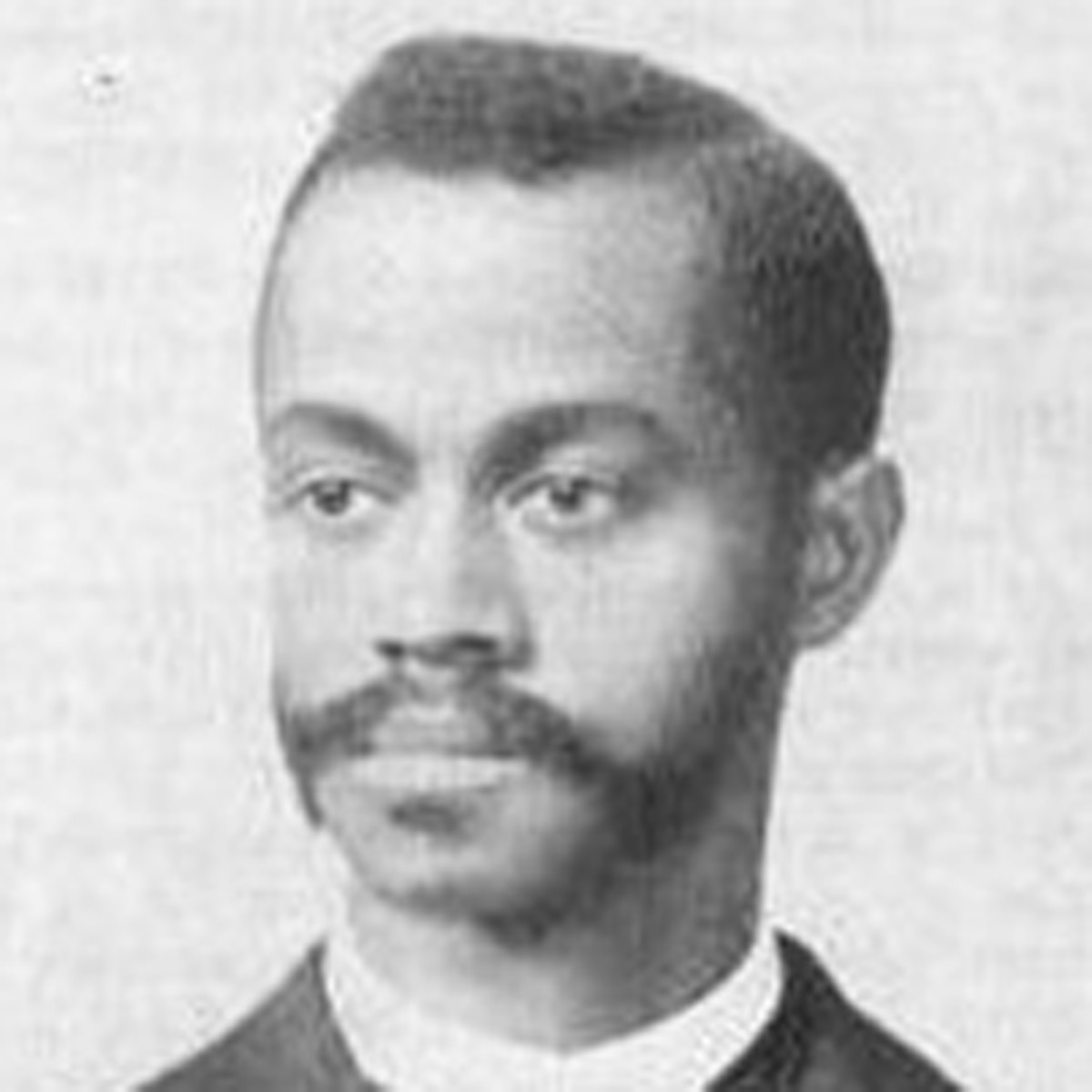 Charles Henry Turner
Charles Henry TurnerCharles Henry Turner was a zoologist, one of the first 3 Black men to earn a PhD from Chicago University. Despite being denied access to laboratories, research libraries, and more, his extensive research was part of a movement that became the field of comparative psychology.
Dr. Turner was a civil rights advocate in St. Louis, publishing papers on the subject beginning in 1897. He suggested education as the best means of combatting racism, and believed in what would now be called a ‘comparative psychology’ approach.
Psychology Month Profile: Penny Corkum
 Penny Corkum
Penny CorkumDr. Penny Corkum studies sleep and children, and created Better Nights Better Days, a cross-Canada trial that improved sleep for both kids and parents before the pandemic. In the last year, Dr. Corkum and her team went back to those families to see how they were doing during COVID. Their launch of a revamped Better Nights Better Days for the pandemic era is imminent.
Standing Committee Releases 2021 Pre-Budget Recommendations (February 2021)
As part of the federal government’s pre-budget consultation process of which CPA contributed to, the House of Commons Standing Committee on Finance released its report. Importantly, two of its top five recommendations focused on investing in a long-term mental health COVID-19 recovery plan for all Canadians, and targeted investments that will improve access to primary care, mental health supports and virtual care. It also included a recommendation to provide a one-time 25% increase in funding to the Tri-Councils for research restart and recovery. Hopefully all three will be reflected in the 2021 federal budget.
Letter to Prime Minister Trudeau and Premier Legault (February 2021)
Given that Prime Minister Trudeau recently signalled the federal government’s willingness to discuss increasing its share of health funding to the provinces and territories, the CPA wrote to the Prime Minister and Premier urging them to increase their investments in mental health services and treatments.
CAMIMIH Letter to Prime Minister and Premiers
Psychology Month Profile: Natalie Rosen
 Natalie Rosen
Natalie RosenBlack History Month: Keturah Whitehurst
 Keturah Whitehurst
Keturah Whitehurst
Psychology Month Profile: Joanna Pozzulo
 Joanna Pozzulo
Joanna PozzuloDr. Joanna Pozzulo and the Carleton University Psychology Department launched a virtual space for researchers, students, and other stakeholders called MeWeRTH (The Mental Health and Well-being Research and Training Hub). It’s a means of connecting the university with community organizations and anyone else who might be a consumer of mental health and well-being research.
Psychology Month 2021 – some of the psychologists doing interesting things during the pandemic
 Some of the psychologists doing interesting things during the pandemic
Some of the psychologists doing interesting things during the pandemic
Meet some of the psychologists who have been profiled in this Psychology Month. We speak with Dr. Adrienne Leslie-Toogood, Dr. Christine Chambers, Courtney Gosselin and Dr. Mélanie Joanisse about their work during the pandemic.
Psychology Month Profile: Vina Goghari
 Vina Goghari
Vina GoghariDr. Vina Goghari is the Editor of the Canadian Psychology journal. The amount of pandemic-related research and article submissions has been overwhelming in the past few months. The upcoming COVID special edition of the journal will present papers that cover a very broad range of topics related to the pandemic.
Psychology Month Profile: Judy Moench
 Judy Moench
Judy MoenchDr. Judy Moench has helped create protocols to help her Alberta community and others during the pandemic. Prepped 4 Learning helps teachers, parents, and kids cope with disruption. The Self-care Traumatic Episode Protocol (STEP) is helping mental health clinicians, hospital staff, and others decrease stress and increase coping.
Psychology Month Profile: Chloe Hamza
 Chloe Hamza
Chloe HamzaDr. Chloe Hamza has an article in the upcoming Canadian Psychology journal COVID-19 special edition entitled ‘When Social Isolation Is Nothing New’. It’s part of an ongoing study of post-secondary students, some of whom had pre-existing mental health concerns before the pandemic, and some of whom didn’t.
“Psychology Works” Fact Sheet: Physical Activity, Mental Health, and Motivation
The Canadian Society for Exercise Physiology (CSEP) recommends that adults aged 18 or older, who do not have a suspected or diagnosed medical condition, do at least 150 minutes/week of moderate-to-vigorous intensity exercise, with each session lasting at least 10 minutes. All adults should also do muscle and bone-strengthening exercises at least twice/week. Older adults (65+) with poor mobility should regularly do activities that help to improve balance and prevent falls (e.g., yoga, tai chi). Women who are or think they may be pregnant, should check pregnancy guidelines with their doctor.
Canadian statistics show that most adults don’t meet these requirements, with levels of physical activity decreasing as people age. Further, statistics show that only 15% of children (5-11 years) and 5% of youth (12-17 years) meet their recommended level of physical activity (60 minutes/day). As children and youth look to adults for behaviours, engaging children in exercise can be helpful to increase the likelihood that these behaviours will become habits that will continue into adulthood.
What Do “Moderate” and “Vigorous” Mean?
The definitions of “moderate” and “vigorous” physical activity depend on your age, health status, current level of activity, and relative level of (dis)ability. For example, a young, able-bodied athlete might not be affected by a brief walk, while an older, generally inactive person with poor mobility might experience this as “vigorously intense.” The following guidelines can help:
- Moderately intense physical activities should noticeably raise your heart rate. While you’re doing moderately intense physical activity, you should be able to have a conversation, but not be able to sing your favourite song.
- Your resting heart rate increases a lot while doing vigorously intense physical activity, although you shouldn’t feel uncomfortable as a result. While doing a vigorously intense activity, you shouldn’t be able to say more than a few words without having to take a breath.
What Are the Mental Health Benefits of Physical Activity?
Regular physical activity comprised of both cardiovascular and resistance exercise, has many mental health benefits. The longer you stick with your exercise schedule and the more often you exercise, the more benefits you’ll see. For example, research shows that regular physical activity can help:
Increase Brain Health
- Boost academic performance (e.g., grades) in children, youth and young adults
- Individuals perform better than others their age on tests of cognitive ability (e.g., memory, attention, processing speed)
- Particularly among middle-aged individuals, reduce the risk of cognitive decline, measured as a slowing in attention, memory, and concentration, later in life
Enhance Wellbeing
- Boost self-esteem, itself a key sign of good mental health and overall wellbeing, from early childhood straight through older adulthood
- Reduce day-to-day stress
- Increase self-reported happiness and lower levels of sadness and loneliness, both in the short-term and later in life
- Reduce feelings of fatigue, improve sleep quality, and lower your risk of insomnia (provided vigorous exercise is not done too soon before bed)
Reduce the impact of Chronic Diseases
- Can reduce symptoms of depression and anxiety and may reduce the likelihood of future depressive episodes
- Improves vascular health, meaning it reduces the risk of stroke, coronary heart disease, atherosclerosis, hypertension, and vascular dementia
- Lowers blood sugar, reducing the risk of developing type 2 diabetes and diabetic complications
- Lower the risk of developing neurodegenerative diseases (e.g., Alzheimer’s Disease) and can make the symptoms of these diseases less severe (e.g., issues with memory, concentration, attention)
- Enhance the impact of the treatment of addictions, particularly in the reduction of cravings
- Aid in the treatment of chronic pain (tailored to your physical abilities), post-traumatic stress disorder, schizophrenia, and body dysmorphic disorders (i.e., being obsessed with a real or imagined physical “flaw”).
Why Does Physical Activity Have These Benefits?
There is no single reason why physical activity has mental health benefits. Instead, research suggests that benefits come from the combined physiological, psychological, social, and neurological effects of exercise.
- Physiological: Physical activity both boosts your body’s production of endorphins and endocannabinoids, which are chemicals that help you to relax, feel more pleasure, and feel less pain, and reduces the amount of cortisol (i.e., “stress hormone”) that your body produces.
- Psychological: Regular physical activity helps to increase feelings of self-esteem and self-efficacy, or how much you believe in yourself to accomplish important goals. Short bursts of exercise can also make you happier in the moment by interrupting negative trains of thought.
- Social: People who exercise regularly tend to have bigger social networks and stronger relationships with friends and family. The regular face-to-face interaction that comes from group exercise (e.g., fitness classes, team sports) boosts your mood and can help to prevent depression.
- Neurological: Physical activity helps your brain to use and produce more dopamine and serotonin, which interact with receptors in your brain that can activate positive emotions. People who exercise regularly also have more blood flow to the brain and reduced inflammation. Exercise stimulates the release of growth factors, which optimize the growth of new blood vessels in the brain, and of existing brain cells. This can be observed as better brain functioning, and some research has found, more brain matter in certain areas (e.g., hippocampus, which is associated with memory).
How Do I Get Started and Stay Motivated?
Before you get started, you should ask yourself why you want to exercise, and what types of exercise might be best for you based on your physical (dis)abilities, personality, and goals. Consult your family physician for help in developing a healthy and realistic exercise plan.
Some of the most common reasons for not exercising include not having enough time, not having enough money, not having enough energy, and feeling uncomfortable (physically or socially). Solutions for these can include:
- Planning to exercise frequently, but in short bursts (i.e., 10 minutes or more).
- Scheduling your day so you exercise when you tend to have more energy, and always try to do what you can.
- Finding free or low-cost activities that you enjoy (e.g., walking, cycling, or pick-up sports).
- Not pushing yourself too hard and trying to find an environment where you feel comfortable and motivated (e.g., home, outdoors, with a buddy).
Once you’ve started your exercise program, there are many ways to help you stick with it. Researchers from numerous areas of psychological research (e.g., clinical, sport, and social psychology) suggest that you:
- Make a plan and set regular, concrete goals.
- Don’t delay.
- Be realistic in choosing and committing to an exercise regimen.
- Remind yourself why exercise is important to you every day and whenever you’re facing difficulties.
- Ensure you eat regular, well-balanced meals and sleep regularly.
- Focus on you and your accomplishments, not what other people are doing.
- Track your progress and celebrate small gains.
- Make physical activity part of your daily routine.
- Don’t do the same thing every time and try to do activities you enjoy.
- Plan for how you’ll deal with potential obstacles or distractions.
- Practice self-compassion, especially when you haven’t met your daily or weekly goals.
- Find an exercise buddy who is similar to you (e.g., age, fitness level, ability level).
Where Can I Go for Help or to Learn More?
Visit the CSEP website for physical activity guidelines: http://www.csep.ca/en/guidelines/get-the-guidelines.
Community and recreation centres offer a variety of programs that can help you add physical activity to your daily routine.
Drop-in sports and fitness classes are a great way to sample what’s available before committing to anything.
See a psychologist to discuss motivational tips, concerns you may have related to self-image and exercising, and strategies specific to your needs.
Where Can I Get More Information?
CPA Sport and Exercise Psychology Section: https://cpa.ca/aboutcpa/cpasections/sportandexercise/
American Psychological Association (APA) Division 47: http://www.apadivisions.org/division-47/
You can consult with a registered psychologist to find out if psychological interventions might be of help to you. Provincial, territorial and some municipal associations of psychology often maintain referral services. For the names and coordinates of provincial and territorial associations of psychology, go to https://cpa.ca/public/whatisapsychologist/PTassociations/.
This fact sheet was originally prepared for the Canadian Psychological Association by Matthew Murdoch, Canadian Psychological Association.
Revised: October 2021
Your opinion matters! Please contact us with any questions or comments about any of the Psychology Works Fact Sheets: factsheets@cpa.ca
Canadian Psychological Association
Tel: 613-237-2144
Toll free (in Canada): 1-888-472-0657
Psychology Month Profile: Laurie Ford

 Laurie Ford
Laurie Ford“Psychology Works” Fact Sheet: Gender Dysphoria in Adolescents and Adults
Temporarily removed, pending updates
“Psychology Works” Fact Sheet: Chronic Pain
What is chronic pain?
Chronic Pain is pain that does not go away. When pain lasts longer than 3 or 6 months, or beyond the usual time of recovery, it is said to be chronic. Different types of chronic pain exist, many of which are not clearly understood. Chronic pain may be associated with an illness or disability, such as cancer, arthritis, or a phantom limb. Some types of pain start after an injury or accident and become chronic over time. Others may begin gradually, as is sometimes the case with low back pain. In some types of chronic pain, like migraine headaches, the pain is recurrent, rather than constant. There are many other kinds of chronic pain, such as postsurgical pain, fibromyalgia, and neuropathic pain. In some cases, the cause of the pain remains unknown.
Research indicates that between 10% and 30% of Canadians experience chronic pain. The direct and indirect costs associated with this are staggering, with estimates in the billions of dollars annually. Women tend to have slightly higher rates of chronic pain than men. People of all ages can experience chronic pain, but it is most common in middle age (for additional information about pain in the elderly, please see the CPA “Chronic Pain Among Seniors” Fact Sheet). Chronic pain can make simple movements hurt, disrupt sleep, and reduce energy. It can impair work, social, recreational, and household activities. People who have been injured in accidents may develop other symptoms, such as anxiety and depression. Chronic pain can have a negative impact on financial security and, in some cases, it can contribute to alcohol or drug abuse. It can also disrupt marital and family relationships.
Pain is invisible. As a result, many people who experience chronic pain feel misunderstood and/or alone in their suffering. Some people feel judged or stigmatized, whereas others believe pain is “all in their head.” Pain is, indeed, “all in the head” because the brain is located in the head, and the origin of pain resides in the brain. Because chronic pain can negatively impact quality of life and functional abilities, it is not surprising that more than a quarter of people who experience chronic pain also experience significant depression or anxiety.
Medications are often used to treat chronic pain. Indeed, medications can help, however, the suitability of long-term use needs to be carefully considered and monitored.
How can a psychologist help a person with chronic pain?
Psychologists focus on many aspects of chronic pain, including assessment, treatment, research, teaching, and advocacy. In terms of treatment, psychologists use several different approaches and techniques to help people with chronic pain improve their quality of life, regain their sense of purpose, and improve their functional abilities. Psychologists address important themes, such as acceptance and loss, and they help people with chronic pain through support, education, and skill building in areas such as relaxation, mindfulness, problem solving, goal setting, sleep, assertiveness, and adaptive thinking.
Cognitive behavioural therapy (CBT) is a form of psychological treatment that focuses on thoughts, feelings, and actions. It aims to help people think and behave in more adaptive ways. Acceptance and commitment therapy (ACT), another psychological approach, focuses on acceptance, choice, and committed action. It aims to help people live in ways that are consistent with their core values. Mindfulness meditation is yet another approach that can help individuals with persistent pain. In all cases, a basic treatment goal is to improve functioning and quality of life, as opposed to eliminating pain symptoms. A vocational assessment examines a person’s interests, aptitudes, and abilities. It can be useful for individuals who may need to change the way they work or the type of work they do. Psychotherapy for anxiety and/or depression can be helpful for individuals experiencing chronic pain, as can treatment for drug or alcohol abuse, when required. Couple, marital, or family therapy can also be beneficial for addressing pain-related interpersonal difficulties.
Are psychological approaches effective?
Numerous scientific studies have demonstrated the effectiveness of psychological approaches in helping people with chronic pain. Psychological treatments have been shown to improve quality of life and functioning in many life domains, such as activities of daily living, emotional health, and interpersonal relationships. Following psychological treatment, people report they are more active, more confident, and more in control of their lives, as well as less depressed and less anxious. In many cases, they endorse reductions in pain and physical symptoms. Even though people may continue to experience pain, it is often more manageable.
Although individual therapy may be offered, people experiencing chronic pain are often treated in groups where they are able to share their experiences with others. Because chronic pain is complex, psychologists frequently work in interdisciplinary or multidisciplinary teams comprised of other health care professionals, such as physiotherapists, occupational therapists, physicians, nurses, and social workers. Again, the primary treatment goal is to help people with chronic pain develop satisfying and healthy lifestyles. Interdisciplinary chronic pain rehabilitation programs are as effective in reducing pain intensity as medications and medical interventions; however, they are more effective in decreasing medication use, reducing health care utilization, improving functional activities, improving mood, and promoting return to work.
How can research help?
In addition to working directly with people who experience chronic pain, psychologists have contributed significantly to our understanding of chronic pain through many types of research. For example, some studies focus on reducing the incidence of chronic pain through injury prevention or early intervention programs. Other studies examine the effectiveness of chronic pain treatments. Some researchers examine how psychological variables influence pain and suffering, whereas others study the role of the central nervous system in a variety of chronic pain conditions.
Where can I get more information?
For information about chronic pain, you could contact the Chronic Pain Association of Canada (www.chronicpaincanada.com) or the Canadian Pain Society (www.canadianpainsociety.ca).
Information about pain in children is available at the web site entitled “Pediatric Pain – Science Helping Children” at Dalhousie University, http://pediatric-pain.ca/ .
Consultation with or referral to a registered psychologist can help guide you as to the use of the therapies mentioned in this Fact Sheet.
You can consult with a registered psychologist to find out if psychological interventions might be of help to you. Provincial, territorial, and some municipal associations of psychology often maintain referral services. For the names and coordinates of provincial and territorial associations of psychology, please visit: https://cpa.ca/public/whatisapsychologist/ptassociations/
This fact sheet has been prepared for the Canadian Psychological Association by Dr. John Kowal, a private practice psychologist.
Revised: January 2021
Your opinion matters! Please contact us with any questions or comments about any of the Psychology Works Fact Sheets: factsheets@cpa.ca
Canadian Psychological Association
Tel: 613-237-2144
Toll free (in Canada): 1-888-472-0657
“Psychology Works” Fact Sheet: Bullying Among Children and Youth
What is bullying?
Bullying among children and youth is defined as repeated, unwanted aggressive behaviour(s) by a youth or group of youths. It involves an observed or perceived power imbalance. It can result in physical, social, or educational harm or distress for the targeted youth.[1]
- The power imbalance may be based on differences in size, strength, ability, popularity, appearance/body size, race/ethnicity, culture, religion, financial resources, sexual orientation, gender identity/expression, or any other difference.
- Bullying is a relationship problem. Over time, the person who is bullying feels more and more powerful and the person who is being bullied feels more and more helpless, shamed, and trapped.
- Bullying requires relationship solutions. That is, solutions that create safety and social-emotional growth for those who bully, those who are bullied, and those who witness it.
- Bullying happens most often when few adults are around (e.g., school playgrounds, hallways, cyberspace).
- At least 1/3 of bullying is experienced beyond school boundaries (e.g., recreation settings, online).
Forms of bullying
- Physical bullying: physical aggression such as hitting, kicking, shoving, stealing or harming property.
- Verbal bullying: teasing, name calling, put-downs, shaming, threatening or humiliating others.
- Social bullying: excluding others, damaging friendships, negative gossiping, spreading rumours etc. This is also known as indirect or relational bullying.
- Cyber bullying: is the use of electronic communication technology to bully others. The technology itself creates a power imbalance. It reaches youth anywhere and at any time, messaging is instantaneous, the audience can be huge, and the messages can be permanent.
How common is bullying?[2],[3]
In 2018, a large and representative sample of Canadian youth in grades 6 through 10 were asked whether they have been involved in bullying over the last two months.
- 36% of the sample reported they had been involved in bullying at least once over this time period.
- 6% bullied others
- 20% were bullied
- 9% reported they both bullied others and were bullied
- Being bullied is more common among girls than boys – approximately 1 in 3 Canadian girls are bullied.
- Bullying others is more common among boys than girls.
- Teasing or name calling is the most common form of bullying for both boys and girls.
- Bullying rates in Canada have remained relatively stable over the last 12 years. Relative to other wealthy nations, Canada ranks in the middle in terms of bullying rates (23rd out of 35 nations).
Bullying – The role of peers
Observational research of elementary school children showed that bullying incidents occurred every 7 minutes on the playground and bystanders were present for 85% of these incidents.[4] Bystanders influence bullying dynamics in both ways:
- When bystanders remain passive observers, this sends the message that bullying is acceptable. The bigger the audience, the longer the bullying incident lasts.[5]
- When bystanders intervene, the bullying stopped within 10 seconds in 57% of observed incidents.[6]
Defending against bullying is a complex, social-emotional task for bystanders. They must recognize the event as bullying, take responsibility for helping, and have the skills necessary to intervene successfully. Research suggests that defending can take multiple forms[7]:
- Comforting: Offering emotional support to the person being bullied.
- Reporting: Telling a teacher or another adult about the bullying.
- Solution-focused: Using assertiveness or problem solving to stop the bullying.
- Aggressive: Using retaliation against the aggressor.
Youth should be encouraged to defend using the behavior that is safest and most effective for them in the moment. Boys tend to defend aggressively and may need help to develop more prosocial intervention strategies[6].
Who is at risk?
Of being bullied?
- Those with few friends who are seen as unable to defend themselves
- Those with a disability, neurodevelopmental difference, special healthcare need, intellectual exceptionality (both gifted and learning disability)
- Overweight children and youth
- LGBTQ children and youth report being bullied significantly more and more severely than other students[8]
Of bullying others?
- Children and youth who believe that bullying is normal
- Those who have friends who bully
- Not all children and youth who bully are alike. Some are popular and socially skilled, while others have behaviour problems and few friends.
Dangers and psychological impacts
Bullying is a health issue. It is linked to both short and long-term mental and physical health problems and academic under-achievement.[9] Strong and supportive relationships with parents, a caring and responsive school environment, and positive relationships with family and friends can all help protect against long-term harm. The harm related to bullying is related to:
- Severity and frequency of the bullying behaviour
- Pervasiveness of involvement in bullying (e.g., is bullying happening in just one relationship or place, or in many relationships and places?)
- Chronicity of involvement in bullying (how long has the bullying gone on? Have there been other bullying problems in the past?)
Children and youth whose bullying involvement has been severe/frequent and/or pervasive, and/or chronic require the most intensive and focused support.
Research has documented many immediate and long-term negative impacts of bullying involvement[10]:
- Negative impacts of bullying are significant and have been found across all cultures.
- For some individuals, the impacts can last throughout life.
- Lessons learned about the abuse of power in relationships from bullying may carry over to: sexual harassment, dating aggression, intimate partner violence, workplace harassment, child and elder abuse.
- Children and youth who both bully others and are bullied tend to have the most severe and enduring problems, including the negative impacts in both lists below.
Negative impacts linked to bullying others[11]
- Depression
- Substance abuse
- Aggression and anti-social behaviour
- Sexual harassment and dating aggression
- Academic problems and increased school dropout rate
- Delinquency and criminal behaviour
Negative impacts linked to being bullied[12]
- Depression, anxiety, mood disorders
- Substance abuse
- Low self-esteem and social confidence
- Isolation and loneliness
- Poor peer relationships
- Stomach aches, headaches
- “Toxic stress” or enduring low grade systemic inflammation which is linked to disease[13]
- School absenteeism and learning problems
- Contemplating, attempting, or committing suicide
How can psychologists help?
In Schools?[14]
- Provide training for staff members on how to promote healthy relationships and social climates, and to identify and address bullying issues.
- After training, teachers report feeling more supportive toward children who are bullied and more confident handling bullying issues.
- Recommend school policies that address prevention, intervention and evaluation. [15]
- Develop intervention strategies for children who are involved in bullying problems that develop social-emotional capacity and skills. Counsel students and families dealing with impacts of bullying and victimization.
Those who bully others?
- Help them recognize and understand the negative impacts of their bullying on others and on themselves.
- Support understanding of human rights to safety, respect, and dignity.
- Help develop the ability to control behaviour, resist peer pressure, and use problem solving strategies.
- Help find ways to use their power in a positive way (e.g., identify leadership roles).
- Find opportunities to engage in positive social experiences with a diverse mix of peers where the focus is on making a contribution to the greater good (e.g., peer mentoring, or peer mediation)
Those who are bullied?
- Help develop an immediate plan of safety so they can feel comfortable attending school and participating in community activities.
- Listen, empathize, and reduce shame and self-blame.
- Help them understand and assert their human rights to safety, respect, and dignity.
- Help find ways to build self-esteem, confidence and healthy interests.
- Find opportunities to form positive friendships with peers.
Bystanders?
- Support understanding of human rights and healthy relationships.
- Educate about bullying and its impacts on health and well-being.
- Use role-play and scripts to teach bystanders specific skills for standing up to various bullying situations, instead of being passive or joining in.
- Run workshops to build assertive communication skills and problem solving skills, and peer pressure resistance.
Where can I get more information?
Additional information about bullying can be found at www.prevnet.ca. For downloadable resources, see Factsheets and Tools for Schools at http://www.prevnet.ca/resources/bullying-prevention-facts-and-tools-for-schools
You can consult with a registered psychologist to find out if psychological interventions might be of help to you. Provincial, territorial, and some municipal associations of psychology often maintain referral services. For the names and coordinates of provincial and territorial associations of psychology, please visit: http://www.cpa.ca/public/whatisapsychologist/PTassociations
This fact sheet has been prepared for the Canadian Psychological Association by Annie Tang, Dr. Joanne Cummings, Dr. Debra Pepler, and Kelly Petrunka, PREVNet. This fact sheet was updated by Dr. Wendy Craig, Dr. Debra Pepler, and Laura Lambe.
February 2021
Your opinion matters! Please contact us with any questions or comments about any of the Psychology Works Fact Sheets: factsheets@cpa.ca
Canadian Psychological Association
Tel: 613-237-2144
Toll free (in Canada): 1-888-472-0657
[1] Centers for Disease Control and Prevention (2014). Retrieved from http://www.cdc.gov/violenceprevention/pdf/bullying_factsheet.pdf.
[2] Craig, W., Pickett, W, King, M. (2020) The health of Canadian youth: Findings from the health behavior in school-aged children study. Public Health Agency of Canada, retrieved from https://www.canada.ca/en/public-health/services/publications/science-research-data/youth-findings-health-behaviour-school-aged-children-study.html#ch10
[3] UNICEF (2020). Canadian companion to the UNICEF report card 16. Retrieved from: https://www.unicef.ca/en/unicef-report-card-16
[4] Craig, W. & Pepler, D. (1997). Observations of bullying and victimization in the schoolyard. Canadian Journal of School Psychology, 2, 41-60. See: http://www.prevnet.ca/sites/prevnet.ca/files/research/PREV-Craig-Pepler-1997-Communique-peers.pdf for a downloadable research summary of this article.
[5] O’Connell, P., Pepler, D., & Craig, W. (1999) Peer involvement in bullying: Issues and challenges for intervention. Journal of Adolescence, 22, 437-452.
[6] Hawkins, D.L., Pepler, D., & Craig, W. (2001). Peer interventions in playground bullying. Social Development, 10, 512-527. See http://www.prevnet.ca/sites/prevnet.ca/files/research/PREV-Hawkins-etal-2001-Communique-peer-intervention.pdf for a downloadable research summary of this article.
[7] Lambe, L. J., & Craig, W. M. (2020). Peer defending as a multidimensional behavior: Development and validation of the defending behaviors scale. Journal of School Psychology, 78, 38-53.
[8] Taylor, C. & Peter, T., with McMinn, T.L., Schachter, K., Beldom, S., Ferry, A., Gross, Z., & Paquin, S. (2011). Every class in every school: The first national climate survey on homophobia, biphobia, and transphobia in Canadian schools. Final report. Toronto, ON: Egale Canada Human Rights Trust. Retrieved from: http://egale.ca/wp-content/uploads/2011/05/EgaleFinalReport-web.pdf.
[9] Hymel, S. & Swearer, S. (2015). Four decades of research on school bullying. American Psychologist, 70, 293-299.
[10] Hymel, S. & Swearer, S. (2015). Four decades of research on school bullying. American Psychologist, 70, 293-299.
See also: Takizawa, R., Maughan, B., & Arsenault, L. (2014). Adult health outcomes of childhood bullying victimization: Evidence from a five-decade longitudinal British birth cohort. Am J Psy in Advance. Retrieved from http://ajp.psychiatryonline.org/data/Journals/AJP/0/appi.ajp.2014.13101401.pdf.
See also: Ozdemir, M., & Stafttin, H. (2011). Bullies, victims, and bully-victims: A longitudinal examination of the effects of bullying victimization experiences on youth well-being. Journal of Aggression, Conflict and Peace Research, 3, 97-102.
[11] Farrington, D.P. & Toffi, M. M. (2011). Bullying as a predictor of offending, violence, and later life outcomes. Criminal Behaviour and Mental Health (21)2, 90-98. See also: Fergusson, D. M., Boden, J. M., & Horwood, L. J. (2014). Bullying in childhood, externalizing behaviors, and adult offending: Evidence from a 30-year study. Journal of school violence, 13(1), 146-164.
[12] Bowes, L., Maughan, B., Ball, H., Shakoor, S., Ouellet-Morin, I., Caspi, A., Moffitt, T.E., and Arseneault, L. (2013). Chronic bullying victimization across school transitions: The role of genetic and environmental influences. Development and Psychopathology, 25, pp 333-346.
13 Copeland, W. E., Wolke, D., Lereya, S. T., Shanahan, L., Worthman, C., & Costello, E. J. (2014). Childhood bullying involvement predicts low-grade systemic inflammation into adulthood. Proceedings of the National Academy of Sciences, 111(21), 7570-7575.
See also: Rueger, S. Y. & Jenkins, L. N. (2014). Effects of peer victimization on psychological and academic adjustment in early adolescence. School Psychology Quarterly, 29, 77-88.
See also: Vaillancourt, T., Hymel, S., & McDougall, P. (2013). The biological underpinnings of peer victimization: Understanding why and how the effects of bullying can last a lifetime. Theory into Practice, 52(4), 241-248.
[14] Pepler, D. & Rodrigues, B. (in press). Bullying prevention: Re-imagining a non-violent and healing learning environment for all students at school. In E. Cole and M. Kukai (Eds.)
Mental Health Consultation and Interventions in School Settings: A Scientist–Practitioner’s Guide, pp. 339-357. Boston: Hogrefe Publishing.
[15] Ttofi, M. M., & Farrington, D. P. (2011). Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. Journal of Experimental Criminology, 7(1), 27-56.
“Psychology Works” Fact Sheet: Quitting Smoking
According to the Canadian Tobacco and Nicotine Survey (CTNS) published in 2022, about 3.5 million people in Canada smoke tobacco. A higher percentage of men (12.9%) than women (9.1%) reported current smoking. In 2022, the prevalence of current smoking among youth aged 15-19 was 4.2% or 89,000. In the same year, the prevalence of current cigarette smoking among young adults aged 20-24 was 7.7% or 185,000. The prevalence of current cigarettes smoking among Canadian adults aged 25 years and older was 11.7% or 3.2 million.[1] Smoking is a leading cause of illness and early death in Canada, reinforcing the need to bring this national smoking rate down even further to allow all Canadians to live longer, healthier lives.
Quitting smoking reduces your chances of developing many physical conditions (e.g., cancers, heart disease, respiratory diseases). Quitting smoking also has a lot of mental health benefits. Compared with those who continue to smoke, people who quit smoking experience the following benefits for many years after quitting: less stress and anxiety; fewer symptoms of depression; more frequent positive emotions; higher overall quality of life; and feeling healthier in general.
Why is Smoking So Addictive?
Nicotine is the major addictive chemical in cigarette smoke and acts very quickly in your body, reaching your brain in about 10-20 seconds. Within about 2 hours of finishing your cigarette, nicotine levels in your body drop by 50%. This leads to cravings, feeling anxious or irritable, and generally feeling ‘down.’
Nicotine affects a number of important chemicals in your brain and body, which can change your mood, make you feel energized, and even reduce pain. However, these effects are short-lived and most common in new or occasional smokers. This is because your body adapts to these changes over time, resulting in a need to smoke more over time in order to feel any of these effects – or just feel ‘normal.’
Although nicotine is very addictive, it’s not the only reason why people have trouble quitting. Lighting up a cigarette is often part of a routine. Whether you smoke after dinner, on work breaks, or when socializing, smoking in response to daily triggers can make it more difficult to quit.
What Treatments Are Available?
Quitting smoking involves managing the physical symptoms and breaking the links between smoking and how you feel, what you do, with whom who you spend time, and how you see yourself. As a result, it often takes many attempts, and many treatment types, before you’re able to quit successfully.
Quitting “cold turkey” is one of the most common approaches, but it’s also one of the least effective. A number of treatments are proven to help make your attempt to quit a success:
- Behavioural Therapy: These treatments target the beliefs, attitudes, and behaviours that support an addiction. Common therapies include cognitive behavioural therapy, acceptance and commitment therapy, and functional analytic therapy.
- Nicotine Replacement Therapy (NRT): NRT comes in two forms: slow release (e.g., nicotine patch) and rapid-delivery (e.g., nicotine gum, inhalers, sprays, patches, lozenges). NRTs help to reduce cravings and withdrawal symptoms by releasing small amounts of nicotine into your body, but are not addictive.
- Prescription Medication: In Canada, two major prescription drugs are used to help people quit smoking: varenicline and bupropion. These drugs affect nicotine receptors in your brain and help to reduce cravings and withdrawal symptoms. Varenicline also helps to make smoking less pleasurable.
Note: You should always consult a doctor for information on the risk of side-effects or interactions before using NRTs or prescription medications.
What Works?
Varenicline is the most effective on its own, but all three types of treatment work. While using at least one of these treatments can boost your odds of successfully quitting by as much as 80%, research shows that the best way to quit is by combining treatments. The two most successful combinations are:
- Combined NRTs, which involve using a combination of a slow-release NRT (e.g., nicotine patch) and a rapid-delivery form (e.g., nicotine inhaler).
- Combined Pharmacotherapy and Behavioural Therapy. You can boost your chances of quitting by using pharmacotherapy (i.e., NRT or prescription drugs) while getting help to quit from a licensed mental health professional (e.g., registered psychologist).
Quit-lines and online help, whether on their own or combined with other treatments, can also increase your likelihood of staying smoke-free.
What Doesn’t Work?
Aversion therapies (e.g., smoking until you feel sick), substituting alternative tobacco products (e.g., chewing tobacco, snuff), and alternative therapies (e.g., hypnotherapy, acupuncture, and natural herbs and remedies) don’t improve your odds of quitting.
What About E-Cigarettes?
E-cigarettes containing nicotine appear to help some people stop smoking traditional combustible tobacco products; however, higher quality research is still needed before widely recommending e-cigarettes for smoking cessation.[2] It is also important to note that switching to e-cigarettes is considered a harm reduction approach, but still has negative health effects compared to stopping all tobacco use.[3]
How Can I Help Myself Quit?
Whatever route you choose, keep in mind that it can be incredibly difficult to quit smoking. Even if it takes you many tries, you can eventually succeed.
Whether it’s your first attempt or your fifth, psychological research shows that there is much you can do to make your quit attempt a success:
- Set concrete and realistic goals (e.g., set a specific ‘quit date’).
- Start using treatments before you quit.
- Tell your friends and family that you’re quitting and let them know how they can help.
- Embrace change in your daily routine, social circle, and motivations.
- Find a buddy who is also trying to quit.
- Gradually reduce your smoking before you quit.
- Start by reducing the amount you smoke.
- Reward yourself, even for small gains.
- Make a plan to deal with withdrawal symptoms (e.g., headaches, sadness, irritability, anxiety) in the first 1-4 weeks after quitting. These are signs that your body is recovering.
- Follow the 4 Ds to help deal with cravings: Distract yourself, Drink water, take Deep breaths, and Delay smoking for as long as possible.
- Get active.
- Keep your focus on what you don’t enjoy about smoking rather than what you enjoy.
- Forgive yourself if you have the occasional cigarette.
- Keep yourself busy.
- Understand your triggers and learn how to manage them.
- Replace cigarettes with other things, activities, and people that you enjoy.
- Re-identify yourself as a “non-smoker” or “former smoker” to your friends, family, co-workers, and yourself.
- Accept that this will be difficult for a while, but the rewards will last a lifetime.
Where Can I Go For Help?
Your family doctor can help you to develop a plan for quitting, figure out which treatments might be most effective, and refer you to other health care professionals who can also help you quit smoking. Doctors can also advise you on the safety of NRTs and medications (e.g., side-effects, interactions).
Registered psychologists can help you develop a plan for quitting and provide therapy that will help you quit. Psychologists can offer a variety of effective therapies and will work with you to figure out which one is likely to work best for you. Check with your provincial or territorial psychological association to find a psychologist in your area who can help you quit smoking.
The Canadian Cancer Society offers a bilingual “Smokers’ Helpline” at 1-877-513-5333. Their telephone counsellors are trained to provide support and help you create a plan for quitting. For more information, visit their website: https://smokershelpline.ca/.
You can consult with a registered psychologist to find out if psychological interventions might be of help to you. Provincial, territorial, and some municipal associations of psychology may make available a referral list of practicing psychologists that can be searched for appropriate services. For the names and coordinates of provincial and territorial associations of psychology, go to https://cpa.ca/public/whatisapsychologist/PTassociations/.
This fact sheet has been prepared for the Canadian Psychological Association by Matthew Murdoch, Canadian Psychological Association. Revised by Sarah Dermody, Ph.D., C.Psych, Department of Psychology at Toronto Metropolitan University.
Revised: July 2025
Your opinion matters! Please contact us with any questions or comments about any of the PSYCHOLOGY WORKS Fact Sheets: factsheets@cpa.ca
__________________
[1] Health Canada. (2022). Canadian tobacco and nicotine survey. https://www.canada.ca/en/health-canada/services/canadian-tobacco-nicotine-survey/2022-summary.html
[2] Levett, J. Y., Filion, K. B., Reynier, P., Prell, C., & Eisenberg, M. J. (2023). Efficacy and safety of e-cigarette use for smoking cessation: A systematic review and meta-analysis of randomized controlled trials. The American Journal of Medicine, 136(8), 804-813. https://doi.org/10.1016/j.amjmed.2023.04.014
[3] Sapru, S., Vardhan, M., Li, Q., Guo, Y., Li, X., & Saxena, D. (2020). E-cigarettes use in the United States: Reasons for use, perceptions, and effects on health. BMC public health, 20(1), Article 1518. https://doi.org/10.1186/s12889-020-09572-x
Psychology Month Profile: Dr. Christine Chambers
 Dr. Christine Chambers
Dr. Christine ChambersDr. Christine Chambers is part of the #ScienceUpFirst initiative, the Scientific Director at the CIHR Institute of Human Development, Child and Youth Health, and many other things. The biggest change for her during the pandemic might be as the Scientific Director of SKIP (Solutions for Kids in Pain).
Black History Month: Dr. Olivia Hooker
 Dr. Olivia Hooker
Dr. Olivia HookerAs a psychologist, Dr. Olivia Hooker worked to change the unfair treatment inflicted upon inmates at a New York State women’s correctional facility. In 1963 she went to work at Fordham University as an APA Honours Psychology professor, and was an early director at the Kennedy Child Study Center in New York City.

Psychology Month Profile: Mélanie Joanisse
 Mélanie Joanisse
Mélanie JoanisseWhen the pandemic began, Dr. Mélanie Joanisse created a simple, easy, and funny Guide to Wellness for her frontline co-workers at the Montfort hospital. It immediately took off and has been shared and translated around the world to help healthcare workers everywhere.
Psychology Month Profile: Khush Amaria
 Khush Amaria
Khush AmariaBlack History Month: Inez Beverly Prosser
 Inez Beverly Prosser
Inez Beverly ProsserPsychology Month Profile: Helen Ofosu
 Helen Ofosu
Helen OfosuBlack History Month: Kenneth & Mamie Phipps Clark
 Kenneth & Mamie Phipps Clark
Kenneth & Mamie Phipps ClarkFebruary is Black History Month and to celebrate and acknowledge the contributions that Black Psychologists have made to the discipline and the world, the CPA will be highlighting historically significant Black Psychologists throughout the month (#BlackHistoryMonth).
Kenneth & Mamie Phipps Clark were psychologists famous for their ‘doll experiment’. Their findings, that even black children showed preference for white dolls from as early as three years old, played a role in outlawing segregation.
Psychology Month Profile: Maya Yampolsky
 Maya Yampolsky
Maya YampolskyThe COVID-19 pandemic has made racism worse around the world for marginalized communities. Racism has made the pandemic worse for those communities as well. Dr. Maya Yampolsky specializes in social and cultural psychology, with a particular focus in her research on systemic racism and how racism enters into our personal lives.
An Interview with Dr. Maya Yampolsky

Dr. Maya Yampolsky spoke to us about the intersection of the pandemic and both structural and overt racism. It was too much to put into just one profile, so we are sharing the whole conversation on Mind Full.
Psychology Month Profile: Karen Blair
 Karen Blair
Karen BlairPsychology Month Profile: Courtney Gosselin
 Courtney Gosselin
Courtney GosselinCourtney Gosselin was one of 25 students from Canada and the UK who worked on the COVID-19 Coping Study between March and August. Part of the study was letters people wrote to their past selves (pre-pandemic) and future selves (what they thought at the time would be post-pandemic).
Psychology Month Profile: Jonathan N. Stea
 Jonathan N. Stea
Jonathan N. SteaThe proliferation of disinformation and misinformation online over the past few years has become more dangerous with the advent of the COVID-19 pandemic. Dr. Jonathan Stea, a clinical psychologist and an adjunct assistant professor at the University of Calgary, is one of two psychologists invited to join Science Up First, an initiative bringing together experts from every field to combat disinformation online.
Psychology Month Profile: Adrienne Leslie-Toogood
 Adrienne Leslie-Toogood
Adrienne Leslie-ToogoodDr. Adrienne Leslie-Toogood works with elite athletes in Manitoba. When the pandemic hit, those athletes were spread out across the world, some unable to return home. In response, Dr. Leslie-Toogood launched the #TerrificTuesdays Zoom therapy sessions, a podcast, a book club, and much more to connect athletes across levels, disciplines, and the world.

Psychology Month Profile: Andrew Ryder
 Andrew Ryder
Andrew RyderDr. Andrew Ryder helped prepare the Fact Sheet ‘Why Does Culture Matter to COVID-19’ for the CPA. An Associate Professor in the Psychology department at Concordia University, Dr. Ryder self-identifies as a ‘cultural-clinical’ psychologist, and the intersection of culture and the pandemic is in his wheelhouse.
Psychology Month Profile: Ian Nicholson
 Ian Nicholson
Ian NicholsonDr. Ian Nicholson is the Manager for Psychology and Audiology at the London Health Sciences Centre (LHSC), and a former President of the CPA. As with most hospitals, the LHSC has had to change many of their practices since early 2020, including the way they deliver instruction as a teaching hospital.
CPA Featured in Benefits Canada Magazine (January/February 2021)
Dr. Karen Cohen (CPA CEO) provided a perspective on whether “employees are being prescribed too much medication for mental-health issues?”
CPA Releases Position Paper on Climate Change and Psychological Science (January 2021)
The CPA recently released a position paper Addressing Climate Change in Canada: The Importance of Psychological Science . The paper has been shared with the Minister of the Environment and Minister of Health.
Psychology Month Profile: Chelsea Moran
 Chelsea Moran
Chelsea MoranChelsea Moran is a PhD student in Clinical Psychology at the University of Calgary. Along with her supervisor Dr. Tavis Campbell, the bulk of her research has been about behavioural medicine – adherence to health behaviours. That research took a fortuitous turn when the pandemic began in early 2020.
Psychology Month Profile: Gabrielle Pagé
 Gabrielle Pagé
Gabrielle PagéPsychology Month Profile: Jenn Gordon
 Jenn Gordon
Jenn GordonDr. Jenn Gordon is an associate professor at the University of Regina, and a Canada Research Chair in the bio-psychosocial determinants of women’s mental health. A study she conducted at the beginning of the pandemic identified a major gap in how women in academia were faring during the pandemic compared to their male counterparts, especially among those with young children.
An Interview with Dr. Steven Taylor

Dr. Steven Taylor of UBC was the first person to identify a need for a comprehensive look at the psychology surrounding pandemics. His book, “The Psychology of Pandemics: Preparing for the next Global Outbreak of Infectious Disease” was published presciently in October of 2019, a month before the first COVID-19 case appeared in Wuhan.